Download
1 / 40
400 likes | 993 Views
A Palliative Approach to Peripheral Vascular Disease/ Gangrene. Connie Sarvis RN, BN, MN, CON(c),IIWCC, CWS, FCCWS Skin and Wound Consultant Seven Oaks General Hospital. Peripheral Vascular Disease. PAD OR PVD ? 12-15% OF ADULTS OVER 50 (THOSE SEEKING HELP) PAIN OR INFECTION .

E N D
A Palliative Approach to Peripheral Vascular Disease/ Gangrene Connie Sarvis RN, BN, MN, CON(c),IIWCC, CWS, FCCWS Skin and Wound Consultant Seven Oaks General Hospital
Peripheral Vascular Disease • PAD OR PVD ? • 12-15% OF ADULTS OVER 50 • (THOSE SEEKING HELP) • PAIN OR INFECTION
Prognosis • Symptoms remain stable in about 15/20 cases • Symptoms gradually become worse in 4/20 cases • Symptoms deteriorate severely in 1/20 cases
RISK FACTORS • Advanced Age • Smoking • Diabetes
Other Risk Factors • Obesity • Sedentary Lifestyle • Stress • Heredity • Diet • Hypertension • Hyperlipidemia • Elevated Blood Glucose • Cardiovascular Disease • Cerebrovascular Disease
CAUSES OF PVD • ATHEROSCLEROSIS • INJURY • INFECTION
Symptoms • Claudication • Pt feels cramping or pain in the back of the calf when walking • As PVD continues to progress, claudication/cramping in the calves occurs even when at rest
Other Pain • If the femoral artery is blocked , then pain may extend up to the thighs and buttocks when walking
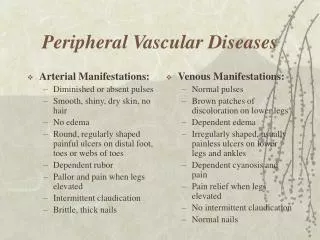
Other Signs and Symptoms • Loss of hair growth on entire leg or in patches • Absent pedal pulses (later stage) • Rubor (later) • Elevation Pallor (Later) • Cool Feet • Delayed capillary refill
ABI’s Measures Vascular Perfusion Doppler Assessment
How is it Measured? • Blood Pressure (Systolic only taken on both arms • Blood Pressure (Systolic only taken on both ankles • Doppler is used (8 mgHz) • Arm – Brachial pulse is used • Legs – Dorsalis Pedis is used
How Do You Get the Number? Formula (ABI) Ankle Pressure Brachial Pressure
But what do the numbers Mean? • Result of <0.5 = Ischemia • Result of 0.5 – 0.8 = Moderate Ischemia • Result of 0.8 – 1.0 = Mild Ischemia/Normal • Anything over 1.0 is either normal or may indicate calcified arteries in Diabetics. • In this case toe pressures are indicated
Why Might Toe Pressure Numbers Differ? Microcirculation vs Macrocirculation!
Results • 55 mmHg = >0.6 toe brachial index (Low Risk) • 40 mmHg = >0.4 toe brachial index (Mod. Risk) • 20 mmHg = >0.2 toe brachial index (High Risk) <20 mmHg = < 0.2 toe brachial index (Severe Risk) If trying to heal an ulcer on the heel, then poor vascularization in the toes is not as critical
BUT…. How do we differentiate between ulcers that will heal and those that need palliative care?
Remember! SKIN IS THE TISSUE MOST RESISTANT TO ISCHEMIA AND SO IS USUALLY THE LAST TO UNDERGO NECROSIS!!
Often times the vascular status is discovered only when trauma occurs and there is not enough vascular perfusion to heal the wound
TREATMENT • Depends upon patient’s condition • Only curative treatment is surgical intervention • Otherwise medical management is preferable
Surgical Procedures • Femoral Popliteal Bypass • Angioplasty • Plaque excision • Stent
Remember!IF SURGERY IS UNDERTAKEN – THERE IS A FRESH BLOOD SUPPLY FOR ANY RESIDENT BACTERIA! = INFECTION!!
Conservative Treatment Cadexomer Iodine and Povidine
Other Measures? • Viagara?? • Low Dose ASA to prevent clots • Statin Medication to lower plaque buildup
GANGRENE • decay of body tissues • caused by infection/ischemia/thrombus • can be black, brown or green • Malodorous!! • Generally associated with Diabetics and Smoking • Frostbite
DRY GANGRENE • BEGINS AT DISTAL PART OF LIMB DUE TO ISCHEMIA • OFTEN IN THE TOES OF ELDERLY PEOPLE • SPREADS SLOWLY • APPEARS BLACK, SHRUNKEN (MUMMIFIED) • PT. HAS DULL ACHE AND SENSATIONS OF COLDNESS • IF CAUGHT EARLY AND REVASCULARIZED – SOMETIMES THE LIMB/DIGIT CAN BE SALVAGED
WET GANGRENE • Generally occurs in moist tissue and organs • Tissue is infected by bacteria which have a putrid smell to them • Develops quickly due to arterial and/or venous blockage • Toxic products of bacteria responsible for sepsis – death.
LOCAL WOUND CARE • Keep wound Dry • Do NOT cleanse with saline first (gangrene) • Do not use Eusol, Saline soaks or Hydrogen Peroxide, Gel’s.
Other Comfort Tips • Avoid tight footwear/binding clothing/dressings • Hang foot down (at night) • Encourage smoking cessation • Avoid trauma
Pain • Fentanyl pre-dressing change • Systemic pain relievers • Gapapentin • Morphine/gel?
Infection • Keep gangrenous/arterial area as dry as possible • Patients very prone to developing osteomyelitis as ulcers can be quite deep • Povidine – Don’t dress until dry • Tightly woven dressings better (no loose fibres)
GOAL • Prevent Pain! • Prevent Infection! • Prevent Amputation!