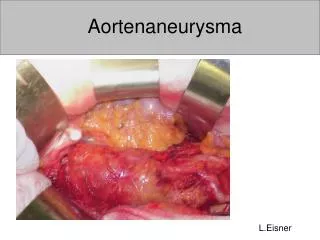
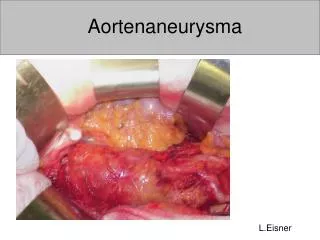
Aortenaneurysma
Aortenaneurysma. L.Eisner. Definition. Aneurysma = Aufweitung > 30 mm > 1.5 x Normaldurchmesser fusiform saccular. Epidemiologie. Prävalenz zw 1.3 – 8.9 % (Männer) Prävalenz zw 1.0 – 2.2 % (Frauen) ca 15000 Todesfälle/Jahr in USA ca 4 rupturierte AAA/Jahr/100‘000

Aortenaneurysma
E N D
Presentation Transcript
Aortenaneurysma L.Eisner
Definition • Aneurysma = Aufweitung • > 30 mm • > 1.5 x Normaldurchmesser • fusiform • saccular
Epidemiologie • Prävalenz zw 1.3 – 8.9 % (Männer) • Prävalenz zw 1.0 – 2.2 % (Frauen) • ca 15000 Todesfälle/Jahr in USA • ca 4 rupturierte AAA/Jahr/100‘000 • Mortalität der Ruptur zw 65 u 85%
Aetiologie • Arteriosklerose • Infektionen: akut: Brucellose / Salmonellose chronisch: Tbc • Entzündlich: Behcet / Takayasu • Bindegewebserkrankungen: Marfan / Ehlers-Danlos
Risikofaktoren • Nikotin • Familiär!Autosomal rezessiv / dominant
Pathophysiologie Degeneration der Arterienwand • Fragmentation elastischer Fasern • Erniedrigung Elastinkonzentration • Proinflammatorische Zytokine • Prostaglandinderivate • MatrixMetalloProtease
Diagnose • Klinik • Sonographie • Computertomographie • MRI
Klinik • Asymptomatisch:palpabel ab ca 5 cm Durchmesser • Diffuse abdominale Symptome • Ruptur
Screening (Sonographie) • Männer 65 -75 mit Nikotinanamnese:Grad B • Männer 65 – 75 ohne Nikotinanamnese:Grad C US Preventive Services Task Force 3/2006
Spontanverlauf AAA • 4 – 5.5 cm: Rupturrate 1% / Jahr • > 6.5 cm. Rupturrate 20% / Jahr • Risikofaktoren: • Weibliches Geschlecht • Durchmesser • Nikotin • Hypertonie • Rasches Wachstum
Therapie asymptomatischer AAA • Prophylaxe der Ruptur • < 4.5 cm: Sono 6 monatlich • 4.5 – 5.5 cm: Sono 3 monatlich • > 5.5cm: Operation / Stent
Risikoevaluation • Rupturrisiko • Anästhesierisiko • Operatives Risiko
Präoperative Abklärung • Computertomographie • (Angiographie) • Kardiologische Abklärung • Ausschluss Malignom! • Lebenserwartung!!
Konservative Therapie • Nikotinstop • Einstellung Hypertonie • MMP Hemmer: Doxicyclin ….
Symptomatische AAA • Diffuse Abdominalbeschwerden • Druckdolentes Aneurysma • Rückenschmerzen
Symptomatische AAA • Dringliche Operation • Intensivmedizinische Überwachung bis zum Eingriff
Rupturierte AAA • Starke Abdominalschmerzen • Starke Rückenschmerzen • Schock (vorübergehende Stabilisierung!)
Rupturierte AAA • Notfallmässiger Eingriff • Abklärung auf Minimum beschränken! • Anästhesiologisches / intensivmedizinisches Monitoring
Offene Operation • Ersatz der Aorta durch ProtheseTube Graft / Y – Graft • Goldstandard
Stent • Anatomie: Proximaler Hals • Endoleak • Langzeitverlauf? • Schlechteste Resultate für grosse AAA • ASA III / IV
Stent • EVAR I: • Teurer • Mehr Komplikationen u Reinterventionen • 3% besseres Aneurysma-bezogenes Überleben • Perspect Vasc Sugr Endovasc Ther 2006 Mar; 18 (1):74EVAR Trial Participants
Stent • Evar II • Relevante 30 Tage Mortalität bei Patienten welche nicht für eine offene Operation qualifizieren • Kein Überlebensbenefit gegenüber konservativer Therapie!! • Perspect Vasc Sugr Endovasc Ther 2006 Mar; 18 (1):76EVAR Trial Participants
Zusammenfassung • Screening bei Risikopatienten (1x Sono) • Operationsindikation ab 5.5 cm (good risk) • Offene Operation bleibt Goldstandard • Stent für selektierte Patienten
Lancet 2005; 365: 1577 – 89 Z Gefässmed 2006; 3 (1) 4 - 8