Download
1 / 68
720 likes | 1.1k Views
Understand endometriosis, adenomyosis, hyperplasia, and carcinoma of endometrium & myometrium. Explore cases and treatment options. Learn about PTEN inactivation and morphological variations. Early diagnosis and management discussed.

E N D
Diseases of Endometrium & Myometrium Prof. C V Raghuveer. Director of PG Studies & Research. II MBBS Combined Lecture 29th July &3rd August 2013
Clinical Vigenette-1 • A 46 yrs old married nulliparous woman -severe lower abdominal pain, virtually in shock. • Menstrual history -Dysmenorrhea. • Emergency U/S -adhesions between ovaries & surrounding structures, no tumor. • R ovary also cystic with semi-solid contents. • Pt recovered from the shock with good conservative management. • What do you think the whole story is about ?
Diseases of Endometrium & Myometrium • Endometriosis: • Presence of endometrial glands/ stroma outside the uterus. • Sites: Ovaries, Uterine ligaments, Rectovaginal septum, Pelvic peritoneum, Laparotomy scars, Umbilicus, Vulva, Vagina, Nasal cavity. Endometriosis can cause Infertility, Dysmenorrhea, Pelvic pain. Endometriotic tissue exhibits excessive inflammatory mediator PGE2 & increased estrogen production due to high aromatase activity in stromal cells. Hence COX-2 and Aromatase inhibitors are useful in treatment.
Theories of Endometriosis • Regurgitation/ Implantation. • Metaplastic. • Vascular/ Lymphatic dissemination Morphology: Endometriosis responds to ovarian hormones resulting in bleeding causing red-blue to yellow brown nodules. Organization & fibrosis result in adhesions. Ovaries develop chocolate cysts & get distorted.
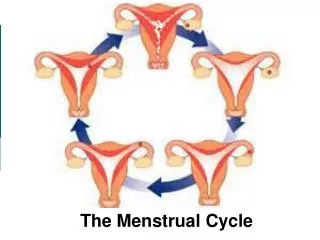
Diseases of Endometrium & Myometrium • Adenomyosis: • Presence of endometrial tissue in uterine wall. • Adenomyosis can cause : • Menorrhagia, • Colicky Dysmenorrhea, • Dyspareunia, • Pelvic pain.
Clinical Vignette-2 • A 40 yrs married woman(para-2)- colicky pain during menstrual periods with menorrhagia ever since she attained menopause. • Clinically bulky uterus. • U/S-enlarged globular, bulky uterus, no tumor. • Pap smear-negative.
Clinical Vignette-3 • A 50 yrs slightly obese lady -metrorrhagia 2 yrs. • Also has flushes now & then. • Clinically – nil significant except pallor. • Pelvic exam -enlarged uterus. • U/S -endometrial cavity uniformly thickened, uterus not shown the degree of atrophy for her age. • Pap smear estrogenic changes. • D&C - histopathology ,benign process. • But hysterectomy had to be done.. • What is this lady suffering from.
Endometrial HyperplasiaEndometrial Intraepithelial Neoplasia • Deserves attention due to its relationship to endometrial ca. • Linked to prolonged estrogen stimulation by anovulation or increased estrogen production. • Conditions promoting hyperplasia : Peri- Menopause, PCOD, Functioning Granulosa Cell tumor of Ovary, Excessive cortical function, Prolonged administration of estrogenic substances.
Role of PTEN IN ENDOMETRIAL HYPERPLASIA & CANCER • Key factor in Hyperplasia & Ca is inactivating mutation of PTEN tumor suppressor gene. which normally blocks Akt phosphorylation in the P13K pathway keeping estrogen in check. Absence of PTEN leads to excessive action of estrogen on glands, causing hyperplasia & ca. • PTEN inactivation seen in 63 % of hyperplasia & 80 % of ca.
Morphology of Endometrial Hyperplasia. Simple,non-atypical/ mild hyperplasia. Irregular glands of various sizes, even cystically dilated. Glands similar to proliferative endometrium. Nuclear stratification is + No nuclear atypia Diffusely affecting endometrium. The lesion rarely progresses & is a response to persistent estrogen stimulation.
Complex/Atypical Hyperplasia 2.Complex/atypical hyperplasia (EIN): Increase in number, size , crowding of glands, increased cell stratification, nuclear enlargement & atypia. scalloped or tufting of epithelium, but glands remain distinct & non-confluent characteristic of EIN. Mitosis common. Severe forms show cytologic & architectural atypia bordering on malignancy Usually focal architectural change.
Morphology & Loss of PTEN Expression in Atypical Hyperplasia & Cancer.A-Simple hyperplasia,B-Atypical ( E I N ), C-Loss of PTEN expression in EIN, D-hyperplasia with squamous metaplasia
Clinical Vignette-4 • A 52 yrs F obese, HT & DM -metromenorrhagia. • Clinically- irregularly enlarged uterus. • Pap -abnormal glandular cells. • U/S-polypoid growth Uterine cavity suspicious invasion myometrium. • What are the possibilities ?
Endometrial Carcinoma • Earlier Cancer cervix was commoner but now, because of early detection & eradication of CIN, incidence of endometrial cancer is becoming relatively more common in younger age groups. • However endometrial cancers are still a disease of post menopausal women.
ENDOMETRIAL ADENOCARCINOMA Incidence: • Peak incidence, 55 to 65 yrs • Uncommon in women younger than 40 yrs • Nulliparous women, late menopause • Obesity, Diabetes mellitus, Hypertension
ENDOMETRIAL ADENOCARCINOMA (CONT’D) Type-1 : Endometrioid Carcinoma. Unopposed estrogen action. Peri-menopausal Upto 85 % of endometrial carcinomas. Risk factors : Obesity, DM, HT, Infertility, Estrogen producing ovarian tumors, HRT, PCOD. Endometrial hyperplasia. Molecular changes: Inactivation of DNA mismatch repair gene & tumor suppressor PTEN gene. • Morphology: Diffuse. Infitrative/exophytic. • Histology: Resembles normal endometrial glands. • But can show differentiation towards: Mucinous, Ciliated, Squamous. • Myometrial, vascular, lymphatic infiltration. Hence stage varies. Grade also varies. I-III. • Prognosis better than Serous type.
Endometrial Carcinoma • Type -2. Serous carcinoma. • 15 % of endometrial cancers. • Much older post-menopausal with an atrophic background. • Morphology: Tufts/ Papillae. • Much more infitrative. • Extra-uterine extension. • More aggressive. • More atypia. • Molecular: High levels of mutant p53+ • Higher stage & grade. • Prognosis worse.
ENDOMETRIAL ADENOCARCINOMA (CONT’D) Morphology: • Localized polypoid tumor • Diffuse tumor • Spread occurs by direct myometrial invasion • Extend to involve endocervix • Later spread to lymph nodes • Histological, Adenocarcinomas
Incidence & Pathogenesis. • Age :55-65 years. • Associated conditions include: • Obesity. • Hypertension. • Diabetes. • Infertility. Two types of endometrial Carcinoma identified: • Those that occur from background of prolonged estrogen stimulation i.e, hyperplasia. • Those unrelated to hyperplasia.
Relationship between Hyperplasia & Carcinoma • Hyperplasia & ca are linked with obesity & anovulatory cycles. • Women with estrogen producing ovarian tumors have a higher incidence of endometrial ca. • Endometrial ca is very rare in ovarian agenesis & in castrated women. • HRT is associated with increased incidence. • Prolonged administration of estrogens to animals have produced polyps, hyperplasia & cancer. • In postmenopausal women there is increased production of estrogens from adipose tissue, adrenal & ovarian androgen precursors explaining occurrence of endometrial cancer in obese & elderly. • Inactivation of PTEN & microsatellite instability are common in hyperplasia & cancer.
The two types of endometrial carcinomas. • Those associated with hyperestrinism & hyperplasia: • Tend to be well differentiated mimicking normal endometrial glands ( Endometroid types) • Differentiation like mucinous, tubal, squamous are more common & they have a more favourable prognosis. • Those not associated with hyperestrinism or hyperplasia: • Occur at a somewhat older age group. • More poorly differentiated. • Resemble ovarian serous carcinoma. • Poorer prognosis, because they spread transtubally & implant on peritoneum. • Infrequently display microsatellite instability & are linked to p53 mutation. • Probably begin as surface tumors & then invade endometrial stroma
Morphology of Endometrial Carcinoma • Gross: 1 Localised polypoid OR 2.Diffuse involving the entire surface. Spread: Direct myometrial invasion & then peritoneal extension to other structures. Spread to regional lymph nodes. Trans-tubal & lymphatic transmission. Distant metastasis to lungs,liver, bones. • Histology: • 85 % are well differentiated , rest are moderately & poorly differentiated. • In 22 % foci of squamousmetaplasia seen which can be benign or malignant- adenosquamous ca or adenoacanthoma. • Serous papillary & clear cell variants have poor prognosis. • Serous types are very aggressive & harbor p53 mutations & accumulate p53 protein.
Staging & Grading of Endometrial Carcinoma • Stage 1: Tumor confined to corpus uteri • Stage 2: Tumor involves corpus & cervix. • Stage 3: Extends outside uterus but not outside true pelvis • Stage 4: Extends outside true pelvis/ involves bladder or rectal mucosa • Grading : each stage can be combined with a grade. • G1-Well diff. • G2-Diff with partly solid areas < 50%, • G3-Predominantly solid or entirely undiff. Serous & Clear cell ca go into G3.
Clinical Course of Endometrial ca • Presentation :Irregular vaginal bleeding with leucorrhea. • Other associated conditions. • Prognosis : depends on stage & grade. • 5year survival for Stage 1 G1-90% after surgery & Rx. • 75 % for Stage 1 G3. • 50 % for Stages 2 & 3. • Serous & Clear cell variants 50 % 3yr survival & 35 % 5 yr survival.
Tumors of Endometrium with stromal differentiation • They comprise < 5 % of endometrial malignancy. • Three types recognized. 1.Carcinosarcoma: Glands & stroma malignant 2.Adenosarcoma: Glands benign, stroma malig. 3. Stromal tumors- starting from benign stromal nodule to stromal sarcoma.
Tumors with stromal differentiation contd 1.Carcinosarcoma: Combination of endometrial adenoca with malingant stromal sarcoma, the latter may in turn differentiate into heterologous elements like muscle, cartilage even osteoid. Clinically similar to endometrial carcinoma. Some pts give past H/O radiation. • Morphologically fleshy, bulky,polypoid, • protruding thro cervical os. • Histology: Combination of adenoca with any type of sarcoma. • Highly aggressive tumors: 5 yr survival is only 25-30 %
Contd 2.Adenosarcoma : Presents as broad based polypoid endometrial growth,protruding thro cervical os. Stroma is malignant & glands benign but abnormally shaped. Seen in 4 th & 5 th decade. • Considered low grade malignant tumors & resemble benign polyps. • Recurrences seen in 25 %. • They are estrogen sensitive & oophorectomy has to be performed hence it is important to distinguish them from benign polyps.
Contd 3.Stromal Tumors : Two categories described. • Benign stromal nodules • Malignant stromal sarcomas. Chromosomal translocation t(7;17) (p15;q21) is common in stromal sarcoma • Stromal nodule is a well circumscribed benign aggregate of stromal cells in the myometrium & does not invade. • Stromal sarcoma is malignant & invasive or invading into lymphatics ( endolymphatic stromal myosis)
Prognosis • Relapse rate : 35% for Stage 1 80 % for Stage 3 & 4. • Distant metastasis may occur many years later. • 5 year survival rate overall is 50 % • Because of chromosomal translocations fusion of JAZFI & JJAZI genes occurs in stromal sarcomas
Myometrial Tumors • Leiomyomas : Also called Fibroids. • Benign tumors of smooth muscle seen in 75 % of women in reproductive period. • Leiomyoma is a clonal neoplasm. • Six cytogenetic abnormalities described. 1.Balanced translocation between Chr 12 & 14. t(12;14) (q14-15;q23-24) 2.Partial deletion of long arm of Chr 7. del(7) (q22q32) 3.Trisomy 12. 4.Rearrangements of 6p,3q, 10q.
Clinical Vignette-5 • A 46 yrs F married, infertile – • dysmenorrhea 10 yrs. • Clinically -pale & weak. • Gynec exam-bulky uterus,irregularly nodular. • U/S -“many circumscribed nodules uterine wall”