ADHS Attentional deficit Hyperactivity Syndrome
ADHS Attentional deficit Hyperactivity Syndrome. Frequency/prevalence. 4 – 6 % of school children more boys than girls About 75 % are affected in adulthood Fixation of a limit is controversial. Symptoms. Attention deficit: distractable, problems to

ADHS Attentional deficit Hyperactivity Syndrome
E N D
Presentation Transcript
ADHS Attentional deficit Hyperactivity Syndrome
Frequency/prevalence 4 – 6 % of school children more boys than girls About 75 % are affected in adulthood Fixation of a limit is controversial
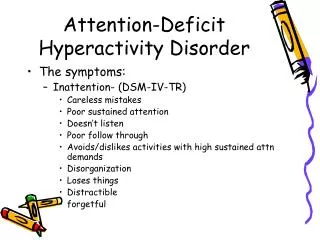
Symptoms Attention deficit: distractable, problems to concentrate, to finish a task Hyperactivity: inability to remain seated talking too much Impuslivity: interrupts other spakers can‘t wait for anything antisocial behaviour No insight into the own disease-state
Cause There is a strong genetic component Speculative: Polymorphism of the D4 gene ??? of the DA-transporter Gene ??? Environmental factors alone can not explain the disease
Psychostimulants in ADHD Amphetamines: Amphetamine (Adderall®)) Methamphetamine (Adderall ®) Methylphenidate (Ritalin ®) Non Amphetamines: Pemoline (Cylert ®) Atomoxetine (Strattera®) Modafinil Under Ivestigation: ABT-418 (N-ACH-R-Ago) S-Citalopram (Escitalopram®, Lexapro®) Histamine H3 receptor antagonists (Komater et al. 2002)
Amphetamin Methamphetamin
Amphetamines: Methylphenidate: Ritalin ®, Medikinet®, Equasym®, Concerta ® Methadate ® D-Amphetamine (D- / S-isomer) Dexedrine ®=Dexamphetamine ®=go-pills for those who do not respond to Ritalin Adderall ® is an amphetamine coctail
Behavioural pharmacology of amphetamine • Self-administered • Dopamine-dependent, mediated by the brain reward system • Dose dependent increase in: • -All behaviours resulting in fragmentation of behaviour • -swichtching – finally stereotypy • Dopamin-dependent, mediated by striatum and N.accumbens • Amphetamine acts rate dependently: • It icreases the response rate of low-rate responder • It decreases the response rate of high-rate responder • („the rate dependency principle“)
Amphetamines in ADHD Rate dependency hypothesis: Children with ADHD are high-rate responders And amphetamines reduce response rates Adults are low rate responders and amphetamines enhance response rates Teicher et al. J Child Adolesc Psychopharmacol 2003, 13: 41-51: „We provide preliminary evidence that methylphenidate exerts rate-dependent behavioural effects (attentiveness) in children with ADHD…..“ „These findings illustrate a clear inverse association between symptom severity and degree of therapeutic response….“
The Yerkes-Dodson-Law Erregungs- Niveau Response-rate
Effect of amphetamine on low-rate responders …….on high-rate responders
Further evidence for the rate dependency principle Children with severe cognitive impairment (IQ less than 45, developmental age less than 4.5 years) react to methylphenidate with increased stimulation/excitation or did not profit from medication. (Handen et al. 1991) Hypothesis: The paradoxical sedating effects of methylphenidate occurs only in high rate responders.
Atomoxetine (Strattera®) Approved in USA and UK for ADHD in children, adolescents and adults. In Germany: March 2005 No psychostimulant drug/ not controlled by BtMG Contraindication: MAO inhibitors Metabolism: P450 pathway: 7 % white 2% black Are poor metabolizers (not dangerous)
Atomoxetine: Mechanism of action Selective noradrenaline reuptake inhibition SNARI Some selectivity for the prefrontal cortex Reboxetine
Atomoxetine effects in humans • Mood brightening, but • no psychostimulant-like high • Neuropharmacology • Enhancement of noradrenaline tone • Facilitates neuronal differentiation during developent • Facilitates neuronal plasticity • protects against various neurotoxins • Behavioural pharmacology • Alerting effects
Atomoxetine in ADHD 1.2 – 1.8 mg /kg /day effective (comparable to methylphenidate) Administration: once daily Approved in the USA for all ages Advantages: see list Disadvantages: see list
Modafinil (Vigil, Provigil, Vigicier, Alertec®) Approved for treatment of narcolepsy Excessive solomnescense Obstructive sleeping-apnoe Controlled by BTM
Modafinil Mechanisms of action α-agonist (prazosin antagonizes some effects) Facilitates Glu-transmission Reduces GABA-transmission Modafinil activates Orexin producing neurons Orexine is a peptide transmitter exclusively originating in the lateral hypothalamus Wakefulness promoting/sleep supressing Orexine deficit is the cause of narcolepsy (Orexine k.o…as a model)
Modafinil effects in humans • Prescribed for narcolepsy, unusual fatigue, • for Parkinsonian patients • Increases vigilance (enhancement in sports) • in US-military, esp. Air Force dexedrine (go-pills) will be replaced by Modafinil • Stimulant, mood brightening • Enhances willingness to work • Meomory enhancing • Compared to amphetamines: Less jitteriness, anxiety, agitation, • no hypersolomescent rebound effect • less peripheral efects • Minimal abuse potential (Rush. et al. 2002, Behav. Pharm. 13:105-115)
Modafinil in ADHD …may be a useful treatment…. When anorexia limits use of stimulants. (Rugino et al. Ped Neurol 2003, 29: 136-142) No rebound upon abrupt discontinuation Improvement in car driving performance Side effects: insomnia
Histamine H3-antagonists in ADHD The H3 receptor is a presynaptic auto- and heteroreceptor It inhibits histamine and Catecholamine release H3-antagonists enhance catecholamine release
Nicotine-R agonists in ADHD Nicotinic ACH-Receptors are located Presynaptically as heteroreceptors on Catecholaminergic terminals Nicotine-R-agonists enhance catecholamine release
Animal models for ADHD Neonatal 6-OH-Dopamine lesion leads to hyperactivity in adulthood (Davids et al. 2002, JPET:301: 1097-1102) Reduced dopamine and metabolite concentration in the striatum (for ex. 90 %) Hyperinnervation due to sprouting by 5-HT neurons Originating in the medial Raphe (for ex. 80%)
Neonatal NMDA-R-anatgonists, cause hyperactivity, • inattention, impulsivity (Fredriksson and Archer 2004) • DAT k.o. • Irrespective of the target addressed: • Many knock-out or knock-in mice exhibit increased • hyperactivity, irritability, impulsivity, aggressivity. • ??? do different neonatal disturbances and compensation processes lead to hyperactivity ???
ADHD in adulthood Untreated ADHD persists in about 66% to Adulthood and results in: adverse/inappropriate/antisocial behaviour addiction.
Stimulant treatment and addiction „Pharmacotherapy of ADHD reduces risk for substance use disorder“ (Biederman et al. 1999) Animal studies Early methylphenidate treatment reduces cocaine brain Reward and stimulation in adulthood ( Mague et al. 2005, Carlezon et al. 2003) Problem: young, but not hyperactive animals have been used
Misuse of ADHD drugs as enhancers For combating sleep For enhacement of motivation for work For mood brightening For cognition enhancement (learning, memory, communication)