Download
1 / 59
590 likes | 1.18k Views
Drug Therapy in the Pregnant Dental Patient. Doreen Matsui MD, FRCPC Associate Professor, Department of Paediatrics Children’s Hospital of Western Ontario. Objectives. To review general principles regarding drugs in pregnancy To describe effects of drugs commonly used in dentistry

E N D
Drug Therapy in the Pregnant Dental Patient Doreen Matsui MD, FRCPC Associate Professor, Department of Paediatrics Children’s Hospital of Western Ontario
Objectives • To review general principles regarding drugs in pregnancy • To describe effects of drugs commonly used in dentistry • To briefly overview use of drugs during breastfeeding
Drug Use in Pregnancy(Larimore WL et al. Prim Care 2000;27:35-53) • 1991 WHO International Survey of Drug Utilization in Pregnancy • 86% of women took medication during pregnancy • Average of 2.9 prescriptions • Despite this high rate of medication intake, most drugs are not labeled for use during pregnancy
Inadvertent Exposure • 1/2 of pregnancies unplanned • Teratogenic potential should be considered and explained to women of childbearing age at time drug is prescribed • <50% of women know they are pregnant by 4th week and ~20% still don’t know by 8th week
Drug Use in Pregnancy(Van Trigt AM et al. Pharm World Sci 1994;16:254-9) • Women interviewed within 2 weeks after delivery • 40% had had one or more questions about drugs during their pregnancy • Similar proportion said that during pregnancy important to consult a health professional before using any medication • Safety was issue that raised the most questions
Compliance • Pregnant women tend to comply less than optimally with drug therapy • Misinformation • 39% of women reported noncompliance predominantly due to hesitation to use drugs during pregnancy (Van Trigt AM et al. Pharm World Sci1994;16:254-9)
Perception of Teratogenic Risk(Am J Obstet Gynecol 1989;160;1190-4) • Women exposed to nonteratogens assigned a risk of 24% for major malformations • Risk in general population 5.6% • May be important factor in decision to terminate pregnancy
Perception of Teratogenic Risk(Sanz E et al. Eur J Obstet Gynecol Reprod Biol 2001;95:127-31) • Perception of risk related to medication used in pregnancy higher than the recognized risk in a group of 15 GPs, 10 gynaecologists, 106 pre-clinical medical students, 150 medical students in clinical training, 81 pregnant women and 63 non-pregnant women
General Considerations • Almost all drugs cross the placenta to some extent • Majority of drugs have not been associated with adverse effects when taken during pregnancy • Weigh therapeutic benefits of drug to mother against its risk potential to developing fetus
Adverse Effects • Spontaneous abortion • Fetal growth retardation • Teratogenicity • Direct drug toxicity • Neonatal drug withdrawal • Long term effects on neurobehavioral development • Carcinogenesis
Teratogenic Risk(Lo et al. Obstet Gynecol 2002;100:465-73) • Standard clinical teratology databases • 485 drugs approved by FDA 1980 - 2000 • Treatment with only small fraction (2.4%) has been associated with substantial teratogenic risk • Took on average 6.0 ± 4.1 years after approval to determine risk
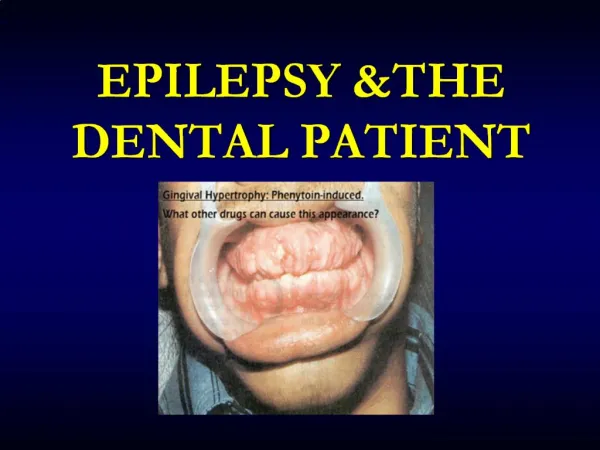
Alcohol (Ethanol) Carbamazepine Cytotoxic chemotherapy DES Isotretinoin and Etretinate Lithium Methimazole Misoprostol Phenytoin Thalidomide Trimethoprim Valproic Acid Warfarin Known Teratogens
Baseline Risk • Risk of major malformation (cosmetic or functional significance) = 3% at birth • Assessment of magnitude of increase in risk above baseline is important • Need to put risk in perspective
Important Factors • Timing of exposure (sensitive period) • “All-or-none” period • *Organogenesis* • “Avoid drug administration, if at all possible during 1st trimester” • Brain development • Dose of drug (threshold, dose-response) • Genetic susceptibility
Associated Factors • Role of underlying maternal disease • Other exposures such as alcohol and cigarette smoking
General Recommendations • Minimize use of medications to those which are necessary and for shortest duration possible • Effective drugs that have been in use for long periods preferable to newer alternatives
Evaluating Risk - Drug Studies • Manufacturer almost never tests product in pregnant women prior to marketing • Evidence from large clinical trials does not exist • Reproductive toxicology studies in animals - extrapolation?
Animals vs Humans • 40-50 chemical and physical agents probably human developmental toxicants • >1200 produce developmental defects in experimental animals • >80% of agents known to produce defects in humans also cause defects in at least one test animal
“CPS” • Majority of drugs not labeled for use during pregnancy • “Safety of Drug X in pregnancy has not been established. Drug X should not be used during pregnancy unless the potential benefit to the patient outweighs the possible risk to the fetus.”
FDA Classification • X, D, C, B, A • Little correlation with risk
Sources of Information • Reference Textbooks • Drugs in Pregnancy and Lactation (Briggs) • Maternal-Fetal Toxicology (Koren) • Computer Databases • Reprotox • TERIS • Teratogen Information Services • Motherisk Program • FRAME Program
The Pregnant Dental Patient • Elective vs urgent • 2nd trimester • Eliminate source of infection or pain • Usually short-term drug therapy
Penicillins • Collaborative Perinatal Project • Frequency of congenital anomalies no greater than expected among children of 4,356 women treated with penicillin (or one of its derivatives) during 1st 4 lunar months of pregnancy
Penicillins and Cephalosporins • Amoxicillin and cephalosporins also considered safe to use during pregnancy • No increased risk of malformations with amoxicillin/clavulanic acid (Clavulin) in 2 studies (Br J Clin Pharmacol 2004;58:298-302 and Eur J Obstet Gynecol Reprod Biol 2001;97:188-92)
Erythromycin • Surveillance study of Michigan Medicaid recipients (1985-1992) • No association between drug and congenital malformations in 6,972 newborns exposed during 1st trimester • Avoid estolate form (cholestatic hepatitis) • Less but reassuring data with clarithromycin and azithromycin
Clindamycin(Scand J Infect Dis 2000;32:579-80) • Hungarian Case-Control Surveillance of Congenital Abnormalities (1980-1996) • OR (95% CI) for clindamycin 1.2 (0.4-3.8) and for lincomycin 1.3 (0.3-5.1) • Limited numbers
Metronidazole • Mutagenic in bacteria and carcinogenic in animals • Small number of reports raised suspicion of teratogenic effect
Metronidazole(Am J Obstet Gynecol 1995;172:525-9) • Outcome of interest = occurrence of birth defects in live-born infants • Overall weighted OR during the 1st trimester calculated by meta-analysis of 7 studies was 0.93 (95% CI 0.73-1.18)
Fluoroquinolones(Antimicrob Agents Chemother 1998;42:1336-9) • Arthropathy in weight-bearing joints of animals • 200 women exposed to fluoroquinolones during pregnancy • Rates of major malformations did not differ between groups exposed to quinolones during 1st trimester (2.2%) and control group (2.6%) • Gross motor milestones did not differ between children in 2 groups
Tetracycline • Main risk is yellow-brown discoloration of teeth • Risk only later than 4-5 months gestation when deciduous teeth begin to calcify • No staining from doxycycline documented • Effects on bone minimal
Local Anesthetics - Lidocaine • Considered relatively safe for use during pregnancy
Epinephrine • Potential to compromise uterine blood flow • Studies have failed to demonstrate adverse fetal effects • Low doses used in dentistry • Avoid inadvertent intravascular injection
Acetaminophen • “Analgesic of choice” • Occasional use at therapeutic doses • Chronic use or overdose
NSAIDS(including Aspirin) • Increased risk of miscarriage? (BMJ 2001;322:266-70) • Gastroschisis (abdominal wall defect) ??? • Avoid use during late pregnancy (3rd trimester) • Bleeding • Inhibition of prostaglandin synthesis • Prolonged labour • Constriction of ductus arteriosus
Studies in fetal lambs demonstrated Celecoxib constricted isolated ductus in vitro Celecoxib produced both an increase in pressure gradient and resistance across the ductus in vivo New COX-2 Inhibitors(Am J Physiol Regul Integr Comp Physiol 2000;278:R1496-505)
Narcotics(Codeine, Oxycodone, etc.) • Don’t appear to risk of birth defects • Low dose short-term regimens acceptable • Respiratory depression • Neonatal withdrawal
Codeine • Unlikely to pose substantial teratogenic risk but data insufficient to state no risk (TERIS, 2002) • Associations between 1st trimester use and congenital anomalies in case-control studies although others have not confirmed • Absence of consistent pattern and criticisms of possible bias in data make it unjustified to consider codeine as causative of these malformations
Nitrous Oxide (N2O) with O2 • Use during pregnancy somewhat controversial • Inhibits methionine synthetase which can affect DNA synthesis • Teratogenic in animals • Single brief maternal exposure during pregnancy unlikely to pose a substantial teratogenic risk • Minimize prolonged use (< 30 minutes, at least 50% O2)
Occupational Exposure to N2O • risk of spontaneous abortion? • Importance of scavenging equipment
Benzodiazepines(BMJ 1998;317:839-43) • Meta-analysis • Cohort studies showed no association between fetal exposure to BZDs and risk for major malformations or oral cleft • Case-control studies showed that risk for major malformations or oral cleft alone was increased • Use around delivery - “floppy infant”
Radiation • In most cases of diagnostic x-rays the fetal radiation exposure is much below the threshold dose of 5 to 10 rad
Average Fetal Exposure Dose(mrad) • Fetal exposure dose from a full mouth series (18 films) or panoramic radiograph is <1/1000 value of concern • 40-fold < naturally occurring background radiation
Antepartum Dental Radiography and Infant Low Birth Weight(JAMA 2004;291:1987-93) • Population-based case-control study • Dental utilization data from Washington Dental Service • Vital record birth certificates from Washington state
Antepartum Dental Radiography and Infant Low Birth Weight(JAMA 2004;291:1987-93) • When thyroid radiation dose was >0.4 mGy (40 mrad), adjusted OR for a term low birth weight infant was 3.61 (95% CI 1.46-8.92) when compared with women with no known dental radiograph Dose to thyroid of dental radiograph 0.08 mGy
Antepartum Dental Radiography and Infant Low Birth Weight(JAMA 2004;291:1987-93) • Weaknesses of study including chance finding and missing data • Criticisms (JAMA 2004;292:1019-21) • Confounding factors • Dental pathology • Radiation dose was related to maternal smoking and late prenatal care • Large # of statistical tests (Type 1 error) • Overestimation of radiation doses
American Dental Association • Abdominal exposure during dental radiography is negligible • Recommend that pregnant women postpone elective dental x-rays until after delivery; however, there are times when an x-ray may be required during pregnancy to help diagnose and treat oral disease (thyroid collar and apron)
Drugs and Pregnancy - Summary • List of drugs which have been associated with adverse effects when taken during pregnancy is relatively short • Teratogenic potential should be explained to women of childbearing age at time drug is prescribed • Lack of information but important to avoid misinformation • Importance of baseline risk
Risk-Benefit Ratio • Benefits of continuing breastfeeding substantial • Convincing reason to justify cessation of breastfeeding required
Clinical Implications • Majority of drugs cross from maternal plasma into breast milk • Most medications found in very small amounts in breast milk (<1% of maternal dose) • Risk of adverse effects in nursing infants is negligible for most drugs