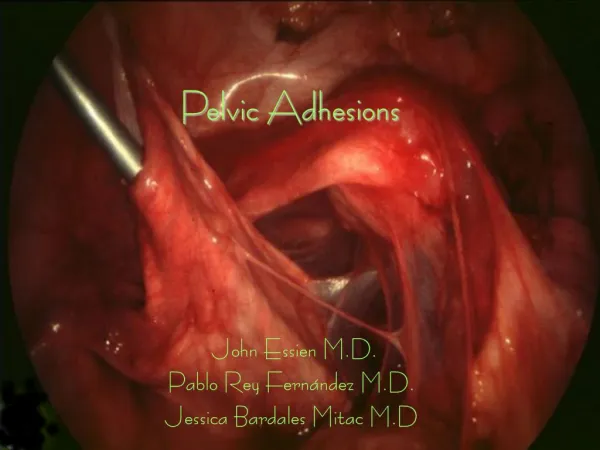
Adhesions
Adhesions. The inflammation and adhesions on and around the dura and spinal nerves are presumed to be the major causes of chronic back pain and radiculopathy. Smyth J, Wright compression on normal nerve root causes paraesthesia and numbness

Adhesions
E N D
Presentation Transcript
Adhesions • The inflammation and adhesions on and around the dura and spinal nerves are presumed to be the major causes of chronic back pain and radiculopathy. Smyth J, Wright compression on normal nerve root causes paraesthesia and numbness compression on injured nerve root causes pain • The lysis of epidural adhesions is considered as one of the effective therapeutic modalities of management of these patients. • The adhesinolysis may be performed either non-endoscopically or endoscopically
History • first attempted using the myeloscope around 1931. • Development of fiber optics and video technology. • The U.S. F DA approved it for visualization of the epidural space in September 1996.
Fluoroscopy Vs endoscopy When fluoroscopic imaging is used alone to direct the steroid injection, judging the distribution of nonionic contrast can be difficult because the fluoroscopic projection is two-dimensional Spinal endoscopy delivers three dimensional color views of investigated tissue in real time. As spinal endoscopy cannot distinguish one level from another . therefore fluoroscopy must be used simultaneously to insure delivery to a specific level.
mechanism of analgesia lavage of algesic substances (e.g., cytokinins, substance P) by saline utilized to enhance optical visualization of the epidural space . stimulation of the neuroinhibitory system by the pulsating effect on the dura and the salutory effect of injection of steroids under direct visualization in the epidural space. more controlled studies needed
Choosing a Modality **MR • Soft tissues T2 – fluid is bright • Multiplanar T1 – fluid is dark -No radiation **CT • Bones – Fluid is dark on CT • Low cost – Acute (clotted) blood is bright • Ubiquitous
Indications for epiduroscopy • Research Epiduroscopy in human autopsy cases has revealeda dorsomedial connective tissue band in the epidural space Kitamura et al showed that repeated bupivacaine injections caused haemorrhage and congestion in the epidural space Igarashi et al showed that In those patients who had received several previous epidural blocks, aseptic inflammatory changes including adhesions were observed.
therapeutic Shimoji et al. were able to identify adhesions and "arachnoid" filaments Spinal cord stimulation electrodes can be placed at the lumbar level under epiduroscopic guidance Schutze G, Groll O It is very difficult to identify the diseased structure in the epidural space when the flexible fibrescope is introduced directly between the spinous processes
Patients suffering from chronic radicular back pain radiating into the lumbosacral nerve root distribution, not responsive to conservative therapy. • Patients with true sciatica with a non-surgical lesion, not responsive to conservative therapy. Indications
Contraindications • Coagulopathy • Pregnancy • Renal insufficiency • Chronic liver dysfunction • History of adverse reactions to local anesthestics or anti-inflammatory drugs • History of gastrointestinal bleeding ulcers • Patients unable to understand informed consent
TECHNIQUE OF EPIDUROSCOPY/SPINAL ENDOSCOPY 17-gauge Tuoghy needle is inserted into the sacral canal guide wire is placed through Tuoghy needle Tuoghy needle is then removed canal passage is widened with 11# scalpel dilator and sheath are passed over the wire The sidearm of the introducer sheath is flushed with 10 ml of normal saline.
The steerable catheter containing fibreoptic cable is passed through the introducer The epidural space is distended with 10 to 15 ml of normal saline The fibreoptic cable along with steerable catheter is introduced The intermittent distension and irrigation of epidural space with normal saline may be required. The total volume of normal saline should not exceed more than 70 ml.
OUTCOMES best outcome is found in cases of monoradicular pain without neurological deficit. A prospective outcome is comparison with use of a single endoscopic procedure to repeat epidural injections would be an important project. Approximately 6000 or more cases have been performed during past five years. No permanent injury has been reported. Pre and post-procedural survey, data indicate a trend toward less opioid medication and improved functional capacity.
Future • It appears the Epiduroscopy will evolve, as arthroscopy and laparoscopy did, to become the diagnostic and therapeutic instrument of choice for many procedures in the spine. Endoscopic procedures have proven to be safer, more effective, and less costly than open surgical procedures; the spine will not be an exception to the fact.