Download
1 / 34
340 likes | 482 Views
Commissioning Challenges for PCTs - shared learning and thoughts from the Southern Cambridgeshire health system. Sally Hind, Chief Executive South Cambridgeshire PCT 30 January 2004. What’s the Southern Cambs Health system’?.

E N D
Commissioning Challenges for PCTs- shared learning and thoughts from the Southern Cambridgeshire health system Sally Hind, Chief Executive South Cambridgeshire PCT 30 January 2004
What’s the Southern Cambs Health system’? Addenbrooke’s main provider: a large acute teaching Hospital, providing DGH and specialist services serves a ‘core catchment’ population of c 230,000; Specialist Services cover approx 1million necklace of Community Hospitals long history of joint working with Addenbrooke’s 8 PCTs in 3 StHA areas and 5 counties working collaboratively
Will share: making our collaborative commissioning arrangements work preparation for Payment by Results from April 2004, with Foundation Trust status of local acute Trust preparation for Choice and managing demand using Care Pathways as a focus for commissioning engaging our clinicians local thoughts on future role of PCTs
Making our collaborative commissioning arrangements work ...
Commissioning structure: Countywide Lead Commissioning arrangements: • Lead Commissioner for each Trust • Supported by: • Cambs Commissioning Leads’ Group“C4” which includes Social Services • County wide Commissioning Leads’ Group“C6” plus Finance Leads’ Group “F6” • County wide Clinical Priorities Forum • Commissioner Leads for the Cancer Network, Ambulance Services, Maternity Services
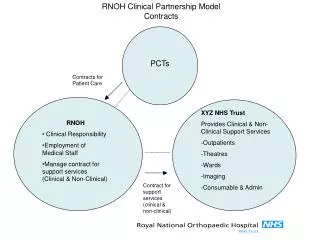
Addenbrooke’s’ Collaborative Commissioning: SCPCT Lead Commissioner for Addenbrooke’s: • Cambridgeshire is 63% of Addenbrooke’s business • Joint Commissioner’s Group around Addenbrooke’s (8 PCTs, Add’s, LSSCG) - Chaired by Uttlesford PCT • SWAP (8 PCTs ) and Addenbrooke’s- performance review • Lead Commissioner mandate; 75% rule for decision making • a Locality Commissioning Manager co-ordinates the process, funded by several PCTs • Chief Executives Addenbrooke’s/SCPCT regular ‘one to one’ sessions
Benefits: • All partners involved • Less bureaucracy with lead arrangements • Pooling of expertise • Improved communication • Risk Sharing • NICE Implementation • Strength in numbers!
Our Learning Points: • recognition of a ‘bigger system’ • need for transparency • building trust between partners • sharing the workload • PCTs have different priorities • application of the 75% rule regarding decision making • representatives must be mandated to take decisions • allowing sufficient time for communication and co-ordination • evaluation and evolution
Preparation for Payment by Results from April 2004, with Foundation Trust status of local acute Trust ...
Our Learning Points re FTs: agree the baseline early: define the baseline: actual, plan or other? agree line on transfers between providers in Networks: agree early what this does to funding below the baseline negotiate with prospective FT what baseline they declare for Purchaser Parity Adjustment partnerships will be under pressure: PCTs will need strategies to retain and strengthen partnership working and avoid returning to an ‘us and them’ culture between provider and commissioner
Our Learning Points re FTs: competition between providers - will have an impact on collaboration and development of Clinical Networks tensions between primary and secondary care - how willing to reduce income by shifts to primary care? work to avoid loss of an open book culture
From here, we’ll be wanting to: explore scope for developing new services where a local acute trust is above national tariff monitor and watch for: over treatment: as additional activity means additional income ‘HRG inflation’: pushing the episode into a more complex category to increase income gaming ! Providers may seek to lessen their WT/WL risks by not declaring ‘surplus’ capacity once overheads covered
From here, we’ll be wanting to: a rapidly falling acute av. length of stay: day case and InP same tariff, so risk of PCT picking up greater rehab bill after swift discharge, so… negotiate reduction in tariff for rehab undertaken by primary/community care refine our Risk Sharing arrangements - essential
Our emerging learning points: Choices pilot - Orthopaedics: 3 PCTs, 5 providers, Ambulance Trust, 134 6m+ waiters Planning for Choice with FTs: model expected flows: anticipate influx from neighbouring areas to specialist teaching trust agree arrangements ‘closing lists’ when it’s clear that waiting lists won’t be met demand management: close engagement of practices re their activity levels seeing spend across all budgets
Choice and demand management: practice utilisation packs practice visits GPSIs (dermatology, orthopaedics, sexual health, vasectomy, ophthalmology, plus others in collab’n with neighbouring PCT) Diabetes Specialist Nurse investigating ‘Frequent Fliers’ Vulnerable People's register Direct Access to Radiology and Pathology training practice experts - Dermatology our monitoring information - you need to identify the problem to tackle it GP referral Audit increased equipment to avoid admission RRT referral protocols....
Working through Care Pathways: • Care Pathways as a framework within which to make commissioning decisions • an holistic focus on the patient: • i.e. not just a series of care spells • Payment By Results asa tool for exercising choicewithin the pathway: • currently only choice for the acute part of the pathway • GMS contract offers scope for choice in primary care • in future, will support choice for community services • currently ‘set price menu’; needs tobe ‘a la carte’
Choice Along the Pathway: Advice Tests & Primary Care re symptoms investigations Management Ongoing Specialist Management Opinion Treatment Follow up and Care • Aiming for Choice to be available at every node along the pathway • Payment By Results (Financial Flows) supports this Choice
Working through Care Pathways: • supports engagement of patients and carers in commissioning decisions: • about the individual’s needs • about the population’s needs • about where investment should be made / new services developed • as a tangible means of involving clinicians • stroke, falls, CHD • slow progress: learning points: • mapping current practice risks reinforcing it ! • no prizes for perfectionism: results are too slow
Engaging our clinicians: • engagement though Care Pathway commissioning - commissioning on specific areas of personal interest and relevance • bringing together across trusts’ organisational boundaries to avoid an ‘us and them’ • harder to fall out over the LDP if our clinicians jointly drove the decisions ! • PBR as the tool to deliver clinicians’ commissioning decisions
Engaging our clinicians…. • Decisions re which quality/other indicators (e.g. distance) should drive ‘Choice’ options: • both GP and hospital clinicians • build the body of information that will inform Choice • engage in understanding the reason for a provider trusts distance from Nat Tariff: • if above - scope for cost improvements • if below - making quality investment decisions
Engaging our clinicians…. Focusing our attention: • Payment by Results = ‘pay as yourefer’ • “...all the money goes into the hospital black-hole”…because that’s where we refer the patients ! • now a direct correlation: we pay for what we send • focus attention on investment in alternatives • clear message to PCTs/GPs that they drive the pattern of investment
What the future holds for PCTs: refocusing on the ‘non contracting’ bits of commissioning up our performance management skills: Foundation Trusts no longer accountable to StHAs through the Annual Accountability Agreement PCTs will need to hone their performance skills for managing their SLAs
And finally Seeing system reform in context...
The key elements of system reform are all complimentary: Choice (the principle)
The key elements of system reform are all complimentary: Payment by Results (the tool) Choice (the principle)
The key elements of system reform are all complimentary: Payment by Results (the tool) Choice (the principle) Foundation Trusts (locally accountable and responsive)
The key elements of system reform are all complimentary: Payment by Results (the tool) Choice (the principle) Foundation Trusts (locally accountable and responsive) Integration (the means to patient focused care)
Underpin with a commissioning framework based on Care Pathways
The key elements of system reform are all complimentary: Payment by Results (the tool) Choice (the principle) Foundation Trusts (locally accountable and responsive) Integration (the means to patient focused care) Pathways (the framework) i.e. Pathways as a tool to commission (planning, service development, ‘contracting’)