Download
1 / 45
580 likes | 1.25k Views
The Beta- Lactamase Family: Classification, Detection, and Interpretive Criteria. COL Helen Viscount, PhD, D(ABMM) LTC Steven Mahlen, PhD, D(ABMM). Transplant patient. Extremely resistant Klebsiella pneumoniae recovered Sensitive only to colistin and gentamicin Patient put in isolation

E N D
The Beta-Lactamase Family: Classification, Detection, and Interpretive Criteria COL Helen Viscount, PhD, D(ABMM) LTC Steven Mahlen, PhD, D(ABMM)
Transplant patient • Extremely resistant Klebsiellapneumoniaerecovered • Sensitive only to colistin and gentamicin • Patient put in isolation • Isolate transmitted to 10 other patients • Outcomes: • 4/5 with bacteremia died • 1 other died • 2 with renal failure • Only 4/11 discharged without renal failure • Ampicillin: R • Pip/tazo: R • Ceftazidime: R • Ceftriaxone: R • Cefepime: R • Imipenem: R • Meropenem: R • Aztreonam: R • Amikacin: R • Tobramycin: R • Trimeth/sulfa: R • Fluoroquinolones: R • Gentamicin: S • Colistin: S
Nursing home resident • 83 years old • Pneumonia • Admitted to ICU • Started on ceftriaxone and levofloxacin • Blood cultures + • K. pneumoniae • Based on sensi’s: • No more levo • Kept on ceftriaxone • Patient got worse • Had to be ventilated • Ampicillin: R • Pip/tazo: S • Cefazolin: R • Ceftazidime: I • Ceftriaxone: S • Cefepime: S • Imipenem: S • Aztreonam: S • Tobramycin: S • Trimeth/sulfa: R • Levofloxacin: I • Ciprofloxacin: I • Gentamicin: S
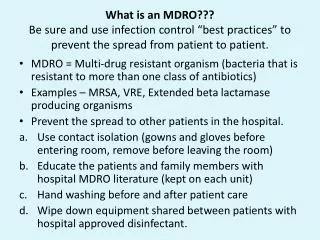
Objectives • At the end of this workshop the attendee should be able to distinguish ESBL positive from carbapenemase-producing bacteria • At the end of this workshop the attendee should be able to describe a method to screen for ESBLs • At the end of this workshop the attendee should be able to interpret the results of the modified Hodge Test
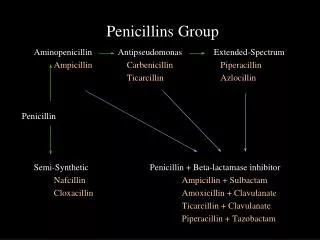
Beta-lactam antibiotics • Penicillins • Ampicillin • Amoxicillin • Piperacillin • Cephalosporins (generations) • 1st gen: cephalothin • 2nd gen (cephamycins): cefoxitin, cefotetan • 3rd gen: ceftazidime, cefotaxime, ceftriaxone • 4th gen: cefepime
Beta-lactam antibiotics • Monobactam: aztreonam • Carbapenems: • Imipenem • Meropenem • Ertapenem • Inhibitors • Sulbactam (ampicillin/sulbactam: Unasyn) • Tazobactam (piperacillin/tazobactam: Zosyn) • Clavulanate (amoxicillin/clavulanate: Augmentin)
Mechanisms of Resistance • Altered target (Gram negative/positive) • Altered permeability (Gram negative) • Production of inactivating enzymes (Gram negative/positive)
Gram-negative cell Gram-positive cell Outer membrane Peptidoglycan Peptidoglycan Penicillin Binding proteins (PBPs) Inner (cytoplasmic) membrane
Alteration of Target • Resistance to -lactams via altered penicillin-binding proteins (PBPs) • MRSA • Vancomycin resistance in enterococci • Fluoroquinolone resistance
Altered Permeability • Passive diffusion of Gram-negative cell wall • Mutate outer membrane proteins • Active efflux
Production of Inactivating Enzymes • Chloramphenicol acetyltransferase • Aminoglycoside-modifying enzymes • -Lactamases
-Lactamases • Well over 340 different enzymes • Extended spectrum -lactamases (ESBLs) • AmpC -lactamases • Chromosomal • Plasmid-mediated • Carbapenemases
-Lactamases • First -lactamase identified: AmpC beta-lactamase • 1940, Escherichia coli • 1940, penicillinase, Staphylococcus aureus • First plasmid-mediated -lactamase: TEM-1 • 1965, Escherichia coli, Greece
H H S R-CONH C C CH3 C N CH3 O COOH -Lactamase Activity -lactam Enzyme-Ser-OH
-Lactamase Activity H H S R-CONH C C CH3 O C N CH3 O H COOH HOH Ser Enzyme
L L L L L L L b-lactamase production L L
Types of Beta-Lactamases • ESBLs • AmpCs • Carbapenemases
ESBLs • Extended-spectrum beta-lactamases (ESBLs) are mutant enzymes with a broader range of activity than their parent molecules • They: • Hydrolyze 3rd and 4th gen cephalosporins and aztreonam • Do not affect cephamycins (2nd gen ceph) or carbapenems • Remain susceptible to beta-lactamase inhibitors
ESBLs • The most common plasmid-mediated ß-lactamases in Enterobacteriaceae are TEM-1, TEM-2, and SHV-1 • TEM: Escherichia coli • Named after first patient with a urinary tract infection that was not treatable with ampicillin • Her name: Temorina • SHV: Klebsiellapneumoniae • “Sulfhydryl variant”; amino acids in the enzyme that cross-link with other molecules • “Classical” ESBLs are derived from TEM and SHV enzymes • “Non-classical” ESBLs are derived from enzymes other than TEM or SHV
Classical ESBLs • Primarily found in E. coli and Klebsiella spp. • Differ from their parent TEM or SHV enzymes by only 1-4 amino acids • >100 TEM- or SHV-derived beta-lactamases have been described – most are ESBLs
Non-classical ESBLs • Many described, but less common than classical ESBLs • CTX-M • Found in multiple genera of Enterobacteriaceae • Preferentially hydrolyze cefotaxime • U.S., Europe, South America, Japan, Canada • OXA • Mainly in P. aeruginosa • Primarily hydrolyze ceftazidime • France, Turkey
ESBL Epidemiology • ESBLs first appeared in Europe in the mid-1980s • Worldwide, but prevalence varies widely geographically and between institutions • U.S. national average for ESBLs in Enterobacteriaceae ~3%
ESBL Epidemiology • ESBL producers especially prevalent in ICUs and long term care facilities • Becoming more widespread in the community also • Have been associated with outbreaks • Typically arise in ICU • Plasmid transfer between GNRs • Organism transfer between patients • Control of outbreaks • Infection control practice – isolation • Restriction of 3rd and 4th generation cephalosporins • Antimicrobial cycling
Clinical Significance • Despite appearing susceptible to one or more penicillins, cephalosporins, or aztreonam in vitro, the use of these agents to treat infections due to ESBL-producers has been associated with poor clinical outcome
Clinical Significance • ESBL genes are often carried on plasmids that also encode resistance to multiple classes of antimicrobials • Aminoglycosides, Fluoroquinolones • Trimethoprim/Sulfamethoxazole • Treatment experience is largely based on classical ESBL producers • Carbapenems • ß-lactam/inhibitor combinations
Typical ESBL Susceptibility Profile • Amp: R • Piperacillin: R • Pip/tazo: S • Cefazolin: R • Cefoxitin: S • Ceftazidime: S • Ceftriaxone: R • Cefepime: R • Aztreonam: S • Imipenem/meropenem: S • Amp: R • Piperacillin: R • Pip/tazo: S • Cefazolin: R • Cefoxitin: S • Ceftazidime: R • Ceftriaxone: R • Cefepime: R • Aztreonam: R • Imipenem/meropenem: S
AmpC: General • Chromosomal • Escherichia coli • Citrobacter freundii • Enterobacter aerogenes, E. cloacae • Serratia marcescens • Morganella morganii • Hafnia alvei • Providencia rettgeri, P. stuartii • Pseudomonas aeruginosa • Aeromonas sp.
AmpC: General • Are not inhibited by -lactamase inhibitors • Normally are repressed, so produced at low levels • Chromosomal: inducible • In all except E. coli • In the presence of certain -lactam antibiotics • Normally, produced at low levels • Plasmid-mediated also
The AmpC of E. coli • Chromosomal, but not inducible • Normally expressed at low levels • Regulated by a growth rate-dependent attenuation mechanism • Can become highly expressed with mutations • Amp: S • Amox/clav: S • Piperacillin: S • Pip/tazo: S • Cefoxitin: S • Ceftazidime: S • Ceftriaxone: S • Cefepime: S • Aztreonam: S • Imipenem/meropenem: S
AmpC Induction and Derepression • Is induction clinically relevant? • True danger—mutation in induction pathway • “Derepressed mutant” • 150-1000 fold more enzyme produced than normal
Chromosomal AmpC profile • Normal • Amp: R • Amox/clav: R • Piperacillin: S • Pip/tazo: S • Cefoxitin: R • Ceftazidime: S • Ceftriaxone: S • Cefepime: S • Aztreonam: S • Imipenem/meropenem: S • Derepressed profile • Amp: R • Amox/clav: R • Piperacillin: R • Pip/tazo: R • Cefoxitin: R • Ceftazidime: R • Ceftriaxone: R • Cefepime: S • Aztreonam: R • Imipenem/meropenem: S
Plasmid-Mediated AmpCs (pAmpC) • First true proof of AmpC on plasmid: 1988 • MIR-1, found in Klebsiella pneumoniae • 90% identical to E. cloacaeampC • Some are also inducible (DHA-1) • Most frequently found in K. pneumoniae • Also commonly found in: • K. oxytoca • Salmonella sp. • P. mirabilis • E. coli, E. aerogenes also
pAmpCs: Distribution • World-wide distribution • Africa, Asia, Europe, Middle East, North America, South America, Central America • CMY-2 is most prevalent globally • Algeria, France, Germany, Greece, India, Pakistan, Taiwan, Turkey, UK, US
Carbapenemases • Carbapenem resistance: • High level production of chromosomal AmpC with decreased outer membrane permeability (porins) • E. cloacae, E. aerogenes • C. freundii • E. coli • S. marcescens • K. pneumoniae (porins)
Carbapenemases • Carbapenem resistance: • Changes in affinity of PBPs for carbapenems • Carbapenemases • Frequently, bugs that produce a carbapenemase produce other -lactamases
Carbapenemases • KPC (plasmid, K. pneumoniae) • “Klebsiella pneumoniae carbapenemase” • IMI-1 (plasmid, E. cloacae) • Nmc-A (plasmid, E. cloacae) • Sme-1 (plasmid S. marcescens) • IMP-1 (plasmid, S. marcescens, P. aeruginosa) • L-1 (chromosomal, Stenotrophomonas maltophilia)
Carbapenemases: Profile • R to carbapenems, penicillins, cephalosporins • S or R to aztreonam, depending on enzyme • So the key: • Look for intermediate or R to imipenem or meropenem!
KPC • Infection control emergency!!! • May test sensitive to carbapenems though! • Extensive multidrug resistance (XDR) • Very rapid spread • Empiric therapy: colistin + tigecycline • KPC 1-8
Further reading • Yang, 2007. Ann. Pharmocother. 41:1427-1435 • Jacoby, 2009. Clin. Microbiol. Rev. 22:161-182 • Black et al, 2005. J. Clin. Microbiol. 43:3110-3113 • Livermore et al, 2001. J. Antimicrob. Chemother. 48 Suppl 1: 87-102 • Pfaller and Segreti, 2006. Clin. Infect. Dis. 42: S153-163.