Download
1 / 38
410 likes | 727 Views
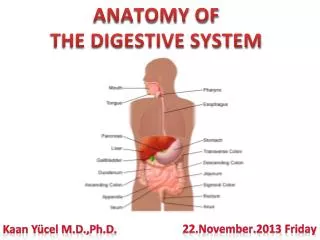
Yeditepe University Medical School Department of Anatomy. ANATOMY OF THE DIGESTIVE SYSTEM PART 2. 9.December.2011 Friday. Kaan Yücel M.D.,Ph.D. LIVER . L argest gland in the body A fter the skin, the largest single organ 2.5 % of adult body weight

E N D
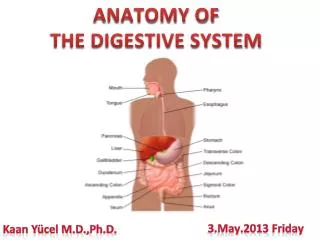
Yeditepe University Medical School Department of Anatomy ANATOMY OF THE DIGESTIVE SYSTEM PART 2 • 9.December.2011 Friday Kaan Yücel M.D.,Ph.D.
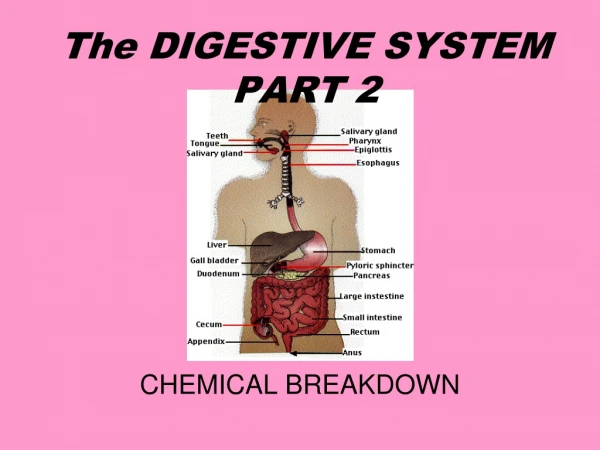
LIVER Largestgland in the body Afterthe skin, the largest single organ 2.5% of adult body weight Except for fat, all nutrients absorbed from the digestive tract are initially conveyed to the liver by the portal venous system. In addition to its many metabolic activities, the liver stores glycogen and secretes bile, a yellow-brown or green fluid that aids in the emulsification of fat.
Bile passes from the liver via biliary ducts—right and left hepatic ducts—join to form common hepatic duct, which unites with the cystic duct to form the (common) bile duct.
The liver produces bile continuously; however, between meals it accumulates and is stored in the gallbladder, which also concentrates the bile by absorbing water and salts. When food arrives in the duodenum, the gallbladder sends concentrated bile through the biliary ducts to the duodenum.
The normal liver lies on the right side and crosses the midline toward the left nipple. Liveroccupies most of the right hypochondrium and upper epigastrium and extends into the left hypochondrium.
Liver has Aconvex diaphragmatic surface (anterior, superior, and some posterior) Arelatively flat or even concave visceral surface (posteroinferior), separated anteriorly by its sharp inferior border that follows the right costal margin.
The diaphragmatic surface of the liver is covered with visceral peritoneum, except posteriorly in the bare area of the liver, where it lies in direct contact with the diaphragm.
Externally, liver is divided into 2 anatomical lobes & 2 accessory lobes by the reflections of peritoneum from its surface, the fissures formed in relation to those reflections and the vessels serving the liver and the gallbladder. These superficial “lobes” are not true lobes as the term is generally used in relation to glands and are only secondarily related to the liver's internal architecture.
The essentially midline plane defined by the attachment of the falciform ligament and the left sagittal fissure separates a large right lobe from a much smaller left. On the visceral surface, the right and left sagittal fissures course on each side of—and the transverse porta hepatis separates: 2 accessory lobes (parts of the anatomic right lobe): Quadrate lobe anteriorly and inferiorly Caudate lobe posteriorly and superiorly.
Gallbladder Liesin fossa for the gallbladder on the visceral surface of the liver. This shallow fossa @ junction of right &left liver.
Relationshipof gallbladder to duodenum is so intimate that the superior part of the duodenum is usually stained with bile in the cadaver. In its natural position the body of the gallbladder lies anterior to the superior part of the duodenum, its neck and cystic duct are immediately superior to the duodenum.
Biliaryducts Conveybile from the liver to the duodenum. Bile is produced continuously by the liver and stored, concentrated in the gallbladder, which releases it intermittently when fat enters the duodenum. Bile emulsifies the fat so that it can be absorbed in the distal intestine.
The bile duct (formerly called the common bile duct) forms by the union of the cystic duct and common hepatic duct. The bile duct descends posterior to the superior part of the duodenum and lies in a groove on the posterior surface of the head of the pancreas.
PANCREAS PANCREAS Elongated, accessory digestive gland that lies retroperitoneally, overlying and transversely on the posterior abdominal wall. Liesposterior to the stomach between the duodenum on the right and the spleen on the left.
The pancreas produces: • Exocrinesecretion (pancreatic juice from the acinar cells) enters the duodenum through the main and accessory pancreatic ducts. • Endocrinesecretions (glucagon and insulin from the pancreatic islets [of Langerhans]) enter the blood. • Pancreasis divided into 4parts: • Head • Neck • Body • Tail
The main pancreatic duct begins in the tail of the pancreas. Main pancreatic duct+ bile duct= hepatopancreaticampulla (of Vater) opens into the duodenum at the summit of Majorduodenal papilla
SPLEEN Ovoid, usually purplish, pulpy mass about the size and shape of one's fist. Relativelydelicate and considered the most vulnerable abdominal organ. Locatedin the superolateral part of the left upper quadrant (LUQ) or hypochondrium of the abdomen where it enjoys protection of the inferior thoracic cage.
As the largest of the lymphatic organs, it participates in the body's defense system as a site of lymphocyte (white blood cell) proliferation and of immune surveillance and response. To accommodate these functions, the spleen is a soft, vascular (sinusoidal) mass with a relatively delicate fibroelastic capsule. The diaphragmatic surface of the spleen is convexly curved to fit the concavity of the diaphragm and curved bodies of the adjacent ribs.
PERITONEUM Continuous, slippery transparent serous membrane. Linesthe abdominopelvic cavity and invests the viscera. Consistsof two continuous layers: Parietal peritoneum lines the internal surface of the abdominopelvicwall Visceral peritoneum invests viscera such as the stomach and intestines.
Peritoneal cavity A potential space of capillary thinness between the parietal and visceral layers of peritoneum Within the abdominal cavity, and continues inferiorly into the pelvic cavity. Containsa thin film of peritoneal fluid, which is composed of water, electrolytes, and other substances derived from interstitial fluid in adjacent tissues.
INGUINAL CANAL Formedin relation to the relocation of the testis during fetal development. An oblique passage approximately 4 cm long directed inferomedially through the inferior part of the anterolateral abdominal wall Liesparallel and superior to the medial half of the inguinal ligament.
Mainoccupant of the inguinal canal Spermaticcord in males Roundligament of the uterus in females
PORTAL SYSTEM Portalvein Finalcommon pathway for the transport of venous blood from the spleen, pancreas, gallbladder, and the abdominal part of the gastrointestinal tract. Formedby the union of splenic vein & superior mesenteric vein posterior to the neck of the pancreas.
Venous drainage of the spleen, pancreas, gallbladder, and the abdominal part of the gastrointestinal tract, except for the inferior part of the rectum, is through the portal system of veins, which deliver blood from these structures to the liver. Once blood passes through the hepatic sinusoids, it passes through progressively larger veins until it enters the hepatic veins, which return the venous blood to the inferior vena cava just inferior to the diaphragm.
VESSELS & NERVES OF THE GASTROINTESTINAL SYSTEM Arich blood supply to support its digestive activities. Arterial blood supplied mainly by Coeliac artery to the stomach, pancreas, spleen and liver Mesentericarteries to the intestines.
Venous blood drains from the stomach, pancreas and spleen via the hepatic portalvein into the liver, where the products of digestion undergo further processing anddetoxification. Blood from oesophagusand rectum does not go through the liver but drainsdirectly into the venous system.
There are two types of nerve supply to the GI tract. The enteric system, found within the walls of the GI tract, is sometimes known as the 'gut brain' and controlsmovement and secretion within the gut.Nerves from the autonomic nervous system also supply the GI tract.
Sympathetic system reduce blood flow to the gut decrease secretions, motilityand contractions, Parasympathetic system Increasein motility and secretion within the tract and relaxation of the gut sphincters. The vagus nerve (Xth cranial) supplies the oesophagus, stomach, pancreas, bileduct, small intestine and upper colon.
Abdominal cavity • Formsthe superior and major part of the abdominopelviccavity. • Has no floor of its own because it is continuous with the pelvic cavity. • Plane of the pelvic inlet (superior pelvic aperture) arbitrarily, but not physically, separates the abdominal and the pelvic cavities. • is the location of most digestive organs, parts of the urogenital system (kidneys and most of the ureters), and the spleen.
More superiorly placed abdominal organs (spleen, liver, part of the kidneys, and stomach) are protected by the thoracic cage. G
Greaterpelvis (expanded part of the pelvis superior to the pelvic inlet) supports and partly protects the lower abdominal viscera (part of the ileum, cecum, and sigmoid colon).
9 regions of the abdominal cavity Regionsare delineated by 4 planes: 2sagittal (vertical) 2 transverse (horizontal) planes
2 sagittal planes Midclavicular(approximately 9 cm from the midline) Midinguinal points midpoints of the lines joining the anterior superior iliac spine (ASIS) and the superior edge of the pubic symphysis on each side.
Two vertical lines Subcostal plane Transtubercularplane inferior border of the 10th costal cartilage iliactubercles (5 cm posterior to ASIS on each side) and body of L5)
Muscles of the Anterolateral Abdominal Wall There are 5 (bilaterally paired) muscles in the anterolateral abdominal wall: 3 flat muscles & 2vertical muscles 3 flat muscles External oblique Internal oblique Transversusabdominis 2 vertical large Rectusabdominis small Pyramidalis The aponeurosesinterweave with their fellows of the opposite side, forming a midline raphe (G. rhaphe, suture, seam), linea alba (L. white line), which extends from the xiphoid process to the pubic symphysis.