Download
1 / 83
850 likes | 1.03k Views
Tailoring Reduced-Intensity Conditioning: Applying Emerging Evidence to Clinical Practice. February 4, 2012 12:15-1:15 pm. Marcos J. de Lima, MD Professor of Medicine Department of Stem Cell Transplantation and Cellular Therapy M.D. Anderson Cancer Center Houston, TX.

E N D
Tailoring Reduced-Intensity Conditioning: Applying Emerging Evidence to Clinical Practice February 4, 2012 12:15-1:15 pm
Marcos J. de Lima, MD Professor of Medicine Department of Stem Cell Transplantation and Cellular Therapy M.D. Anderson Cancer Center Houston, TX
Faculty Disclosures Marcos J. de Lima, MD Professor of Medicine Department of Stem Cell Transplantation and Cellular Therapy M.D. Anderson Cancer Center Houston, TX Research Grant – Celgene Kaci Wilhelm, PharmD Clinical Pharmacy Specialist Blood and Marrow Transplant M.D. Anderson Cancer Center Houston, TX No relevant financial relationships to disclose
Agenda 12:15-12:45 p.m. Critical Decisions: Pretransplant Conditioning - Marcos J. de Lima, MD 12:45-1:05 p.m. Putting the Evidence into Practice: Optimized Dosing and Administration of Reduced-Intensity Conditioning Regimens - Kaci Wilhelm, PharmD 1:05-1:15 p.m. Faculty Panel: Questions & Answers
Critical Decisions: Pretransplant Conditioning Marcos J. de Lima, MD M.D. Anderson Cancer Center Houston, TX
Discussion Topics • Historic perspective and definitions • Donor and recipient-related covariates that influence transplant outcomes and regimen choice • Myeloablative versus reduced intensity regimens – can we really compare them ? • Donor – recipient issues that influence regimen choice • We may not need to reduce dose intensity for all patients in the 6th and 7th decade of life • Conclusions
Goal of Preparative Regimen • Immunosuppression - adequate to prevent rejection • Cytoreduction - eradicate or control malignancy (this element not needed if disease is controlled by prior therapy) • Stem cell space (not myelosuppression) - allow donor cells to compete effectively
05/22/11 06/09/11 07/06/11 08/04/11
How did we get here? • 1922, Fabricious-Moeller • Shielding of legs of guinea pigs during TBI decreased myelosuppression. • 1952, Jacobsen/Lorenz • Protection of TBI aplasia by injection of spleen cells from syngeneic mice. • 1956, Nowell/van Bekkum/Ford/Tausche • Concept of radiation chimera.
Head of a Lion, the Mid-section of a Goat and the Hindquarters of a Dragon http://wpcontent.answers.com/wikipedia/commons/thumb/b/b3/Chimera_Apulia_Louvre_K362.jpg/180px-Chimera_Apulia_Louvre_K362.jpg
BMT Landmarks • 1955, Barnes and Loutit • Carcinoma bearing mice exposed to lethal TBI with syngeneic spleen cell transplantation had long lived protection, but 50% of mice receiving allogeneic spleen cells died before day 100 without tumors. GVL and GVHD. • 1958, Santos • Lymphocytes (T-cells) mediate GVHD, and target organs are lymphoid, skin, gut, and liver.
100 80 60 40 20 0 Two-year Probability of Treatment-related Mortality After Transplants for CML, 1992-1997 < 20 years 20 – 40 years > 40 years 62% 53% PROBABILITY, % 41% 38% 27% 17% 11% 11% 9% HLA-ident Sib Unrelated Auto Leukemia TOS00_13.ppt
1990’s: How to improve treatment-related mortality and morbidity? • Improvements in supportive care, antibiotics, blood support, etc. • Decrease the dose ?
Graft-vs-Malignancy Allogeneic SCT • Much of the benefit of alloSCT is due to immune GVL effect; therefore maximally ablative therapy may not be needed. • Lower dose nonmyeloablative preparative regimens may be sufficient to prevent rejection. • It was hypothesized that a reduced intensity, nonmyeloablative allogeneic transplant could reduce toxicity and allow successful treatment of older patients and those with major comorbidities.
ASH-Orlando 1996 MDACC Hadassah Seattle
Graft-versus-Leukemia Effect (GVL) • Intrinsic disease susceptibility is different. • Some diseases need more chemo / radiation dose intensity than others.
Graft-versus-Leukemia Effect (GVL) • + + + + Low grade lymphomas, chronic myeloid and lymphocytic leukemias. • + + Myelodysplastic syndrome and acute myelogenousleukemia. • + Acute lymphocytic leukemia.
Histocompatibility Intensity
Review Question: Regarding the graft-versus-leukemia effect, it is true that: • Donor neutrophils are the effector cells. • Chronic myelogenous leukemia is more sensitive to the graft-versus-leukemia effect than acute lymphoctye leukemia. • It is not influenced by the use of systemic steroids. • It is rarely associated with graft-versus-host disease.
Review Question: Regarding the graft-versus-leukemia effect, it is true that: • Donor neutrophils are the effector cells. • Chronic myelogenous leukemia is more sensitive to the graft-versus-leukemia effect than acute lymphoctye leukemia. • It is not influenced by the use of systemic steroids. • It is rarely associated with graft-versus-host disease.
Definitions Bacigalupo A, et al. Biol Blood and Marrow Transplant 2009.
Myeloablative Dosing Thresholds Total dose per course Busulfan equivalent dosing: 7.2mg/kg IV or 288mg/m2 Giralt S, et al. Biol Blood Marrow Transplant 2009; Madden T, et al. Biol Blood Marrow Transplant 2007.
Engraftment Graft Host Stem cell dose T-cell dose Graft-facilitating cells Stromal stem cells? Immunosuppression Preparative Regimen Post transplant Rx Disease effects Sensitization Histocompatibility
Patient-related Variables • Age • Comorbidities • Performance Status • CMV Status • Other Infections
Hematopoietic Cell Transplantation-Comorbidity Index (HCT-CI) for Non-Relapse Mortality (NRM) and Survival after Allogeneic HCT Sorror M and Collaborators Fred Hutchinson Cancer Research Center, Seattle, WA and MD Anderson Cancer Center, Houston, TX
Diagnosis is AML in First Remission - Individual Comorbidities % of patients Lung Liver Cancer Cardiac Obesity Infection DM Psych Rheum
2-year NRM Stratified by HCT-CI Scores Score 3 Score 1-2 Score 0 MDACC FHCRC Percent NRM 37 27 19 21 7 7 Years after HCT
Score 0 Score 1-2 Score 3 Two-year Survival Stratified by HCT-CI Scores FHCRC MDACC Percent survival Years after HCT
• Genetics• Social economic issues• Access to treatment Race
Disease-related Variables • Previous treatment(s) • Marrow microenvironment • Susceptibility to the GVL effect • Disease tempo
- Donor-recipient ABO compatibility- CMV- Parity - Age (??)- Availability- Co-morbid conditions Donor-related Variables
Graft • Several institutional and/or investigator biases. • Donor choice (marrow versus PBPC). • PBPC may be a better choice with reduced intensity preparative regimens. • De novo chronic GVHD with PBPC is a serious problem. • ASH 2011: results of randomized PBPC versus marrow in unrelated donor transplants.
Donor Type Cord Blood versus Unrelated Marrow or Peripheral Blood Stem Cell
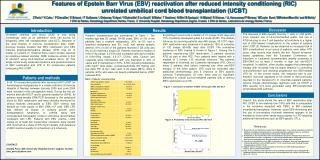
Effect of Graft Source on Unrelated Donor Haemopoietic Stem-Cell Transplantation in Adults with Acute Leukemia: A Retrospective Analysis N=1525 - transplanted between 2002 – 2006 UCB = 165 PBPC = 888 Bone marrow = 472 All myeloablative Diagnoses: AML and ALL Eapen et al. Lancet Oncol 2010.
Probability of Leukemia-Free Survival for Patients IN REMISSION NOT IN REMISSION Eapen et al. Lancet Oncol 2010.
Donor Recipient
Anti HLA Antibodies Anti B13, B27, B38, B39, B41, B45, B49, B50, DR7, DR9, DR53, DQ2, DQ8, DP1, DP11, DP13, DP15, DP17, DPB1*02:02 The patient's serum has reactivity against HLA-DPB1*09:01 (827 MFI).
Unrelated Donor Transplants at MDACC Are we there yet? NO!! Median age of AML Patients: mid 60’s. MDS: mid 70 - late 70’s




![[Ebook] Sensory Integration: Applying Clinical Reasoning to Practice With Diverse](https://cdn7.slideserve.com/12483678/slide1-dt.jpg)