Download
1 / 32
330 likes | 464 Views
Explore current treatment options and the introduction of two new methods for managing varicose veins. Learn about the mechanisms, clinical trials, and future treatment approaches. Compare thermal and non-thermal methods, such as MEchanochemical ablation. Discover the benefits, success rates, and limitations of these advanced techniques.

E N D
Management of Varicose VeinIntroduction of new technology Wong Wing-Fu Ivan Tuen Mun Hospital
Content • Current treatment options of Varicose Vein • Introduction of two new methods • Mechanism • Clinical Trial • Conclusion of future treatment approach
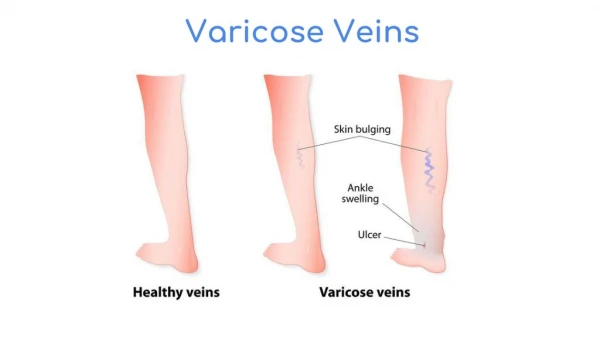
Background • Dilated, tortuous, palpable superficial vein with reversed blood flow • ~30%population • More in Female • Symptoms • Pain, itching, skin pigmentation • Bleeding • Venous ulcer
Treatment • According to NICE guideline 2014 • Intervention therapy • Compression • Surgery • Endovenous ablation • What news
Endovenous therapy • Thermal Tumescent (TT) • Endovenous RadioFrequency ablation (RFA) • Endovenous laser ablation (EVLA) • Endovenous steam ablation (EVSA) • Non-Thermal Non-Tumescent (NTNT) • Chemical ablation • Mechanochemical ablation
Thermal tumescent (TT) • Duplex USG localization and greater saphaneous vein (GSV) identified • Catheter introduced • Injection of Tumescent solution (diluted local anesthesia) • Mixture of normal saline + lignocaine with adrenaline + sodium bicarbonate • Heat sink • Separate GSV from saphenous nerve • Contraction of vein
Mechanism • RFA • Denaturation of collagen matrix • Causing injury to vein wall • Fibrotic sealing of vessel lumen • EVLA • Direct causing carbonization of vein wall • Formation of steam bubbles and transmit heat energy to endothelium • Thrombosis and occlusion of vein
Compare to surgery • Similar success rate to surgery • Less post-operative pain • Less complication • Early return of work • Better quality of life
Endovenous steam ablation (EVSA) • First report in 2011 • Steam vein sclerosis (SVS) system • Apply thermal energy (steam micro-impulse) • Sterile water was heated up and transferred into vessel lumen via catheter • Endothelial damage, result in lumen obliteration and fibrosis • 60J/ cm/ pulse
EVSA - Procedure • Steam ablation catheter (diameter 1.2mm) cannula into vein • Positioned 2-3cm distal to SFJ • Tumescent anesthesia administered • Steam pulses was delivered according to vein diameter and withdrawn by 1cm each time • 2pulses/cm <7mm, 3pulses/cm 7-10mm, 4pulses/cm >10mm
Phase II study • Safety analysis: No major complication • Obliteration rate: 96% at 6 months and 12 months
Compare EVSA vs EVLA • Primary outcome • Treatment success at 12 weeks and 52weeks (obliteration of GSV segment and absence of reflux) • Change in Venous Clinical Severity Score (VCSS) at 12 weeks
Relatively similar successful rate • Primary Outcome • EVSA not inferior to EVLA
Better pain control and less limit in daily life • Secondary Outcome
EVSA • Benefits • Using sterile water not inducing harm by generating exogenous substance • Stable, constant and relatively low peak temperature • Fewer temperature-related symptoms (pain and bruising) • More thin and flexible fiber • no need guidewire • Feasible to more tortuous vein • Limitations • Lack of large scale high quality study • Still need further study compareEVSA to RFA/ surgery
Limitation of TT • Need for tumescence multiple injection • Risk for thermal injury • Post-operative pain • Need of generator (cost of money)
Non-Thermal, Non Tumescent (NTNT) • US guided foam injection (USGF) • Chemical ablation • Sodium tetradecyl sulphate (STS)/ Polidocanol • Induce fibrosis and inflammation • Result in lumen obliteration • Limitations • 2.4 folds of primary failure compare to surgery group
USGF • More adverse events • Skin staining/ pigmentation • Persistent lumpiness • Cough • Chest tightness • Myocardic infarction • Risk of neurological events • Headache • Transient visual disturbance • Stroke
Non-Thermal Non-Tumescent (NTNT) • Mechanochemical ablation (MOCA) • First reported in 2012 • Hybrid system • Infusing liquid sclerosant • Rotating a wire within lumen at 3500rpm • Abrade the intima allow better efficacy of sclerosant • Mix sclerosant in vein and onto vessel wall • Catheter tip at 2cm distal SFJ • Pull down rate 1-2mm/second
Mechanochemicaltumescentless endovenous ablation: final result of initial clinical trial • Primary outcome • Safety, follow-up to 6 months • No severe adverse events • No neurological events • Primary closure rate • 96.7% (29/30) • Secondary Outcome • Pain control • No complaint of pain during procedure and follow-up • Use of analgesia • Only Local anesthesia given during procedure • Presence of ecchymosis • 10% (3/30)
Prospective observation study • Less post-op pain 100-mm visual analog scale (14 days) • 4.8 vs 18.6 (p<0.01)
Mechanochemical ablation (MOCA) • Earlier return normal daily activities and work resumption • Similar improvement in quality of life questionnaires
Mechanochemical ablation (MOCA) • Benefits • No thermal related injury • No need of multiple tumescent injection • Simple and faster procedure • Limitations • Lack of high quality clinical trial • Ongoing study • MOCA Versus RFA in the Treatment of Primary GSV incompetence (NCT01936168)
Conclusion - Meantime • New treatment options still need more high quality clinical trial • Current treatments are improving • Endovenous treatments achieve similar efficacy as surgery with less adverse events • NICE recommend endothermal ablation as first choice if patient is suitable
Conclusion - Future development • More use of minimal invasive procedure • Efficacy relative similar among them (>90%) • Focus on cost-effectiveness, improve in quality of life • Surgery is still important • patient not suitable for endovenous treatment • Office-based procedure • Procedure done in clinic • No hospital stay • Short procedure time • More patient being treated, less waiting time
Reference • A Systematic Review and Meta-analysis of Randomised Controlled Trials Comparing Endovenous Ablation and Surgical Intervention in Patients with Varicose Vein, B. Siribumrungwong, European Journal of Vascular and Endovascular Surgery 44 (2012) • Systematic review of foam sclerotherapy for varicose veins, X. Jia , British Journal of Surgery 2007 • A Randomized Trial Comparing Treatments for Varicose Veins, Julie Brittenden, M.D., The new england journal of medicine 2014 • Randomized clinical trial of endovenous laser ablation versus steam ablation (LAST trial) for great saphenous varicose veins, R. R. van den Bos, British Journal of Surgery 2014 • Endovenous therapies of lower extremity varicosities: A meta-analysis, Renate van den Bos, JOURNAL OF VASCULAR SURGERY January 2009 • Great Saphenous Vein Ablation with Steam Injection: Results of a Multicentre Study, R. Milleret, European Journal of Vascular and Endovascular Surgery 2013 • Mechanochemical tumescentless endovenous ablation: final results of the initial clinical trial, S Elias, Phlebology 2012 • Postoperative pain and early quality of life after radiofrequency ablation and mechanochemical endovenous ablation of incompetent great saphenous veins, Ramon R. J. P. van Eekeren, JOURNAL OF VASCULAR SURGERY February 2013 • Proof-of-principle study of steam ablation as novel thermal therapy for saphenous varicose veins, Renate R. van den Bos, JOURNAL OF VASCULAR SURGERY January 2011 • Ultrasound-guided foam sclerotherapy is a safe and clinically effective treatment for superficial venous reflux, Andrew W. Bradbury, JOURNAL OF VASCULAR SURGERY October 2010 • Temperature profiles of 980- and 1470- nm endovenous laser ablation, endovenous radiofrequency ablation and endovenous steam ablation , Lasers Med Sci (2014) • http://clarivein.com/ • https://www.youtube.com/watch?v=hnNMdkUy_0w • National Institutefor Health and Care Excellenc guideline 2014