Download
1 / 25
250 likes | 449 Views
PANEL DISCUSSION SURGERY FOR CROHNS DISEASE. AD 24 female. Crohns disease since 2001 on penatasa, budesonide, prednisolone needle phobia resolved by psychologist onto azathioprine October 2004 – wt loss, colicky abdominal pain on eating barium meal and follow through. AD 24 female.

E N D
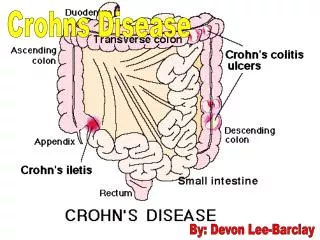
PANEL DISCUSSION SURGERY FOR CROHNS DISEASE
AD 24 female • Crohns disease since 2001 • on penatasa, budesonide, prednisolone • needle phobia resolved by psychologist onto azathioprine • October 2004 – wt loss, colicky abdominal pain on eating • barium meal and follow through
AD 24 female Barium Meal and F/T - Featureless terminal ileum over 15cm with a very tight stricture at the ileocaecal valve over a very short distance • no previous surgery • BMI 18 WHAT NEXT ?
AD 24 female LAPAROSCOPIC RESECTION • laparoscopic resection – ileocaecetomy 25cm specimen • stapled anatomosis • postoperative ileus • home on day 10
KH 38 female nurse • Crohns disease for 17 years involving the terminal ileum managed with azathioprine and steroids • August 2003 – IP subacute obstruction
KH 38 female nurse • BM & F/T “long segment of strictured terminal ileum - ? Early filling of sigmoid and rectum ?? Fistula
KH 38 female nurse • September 2003 OPD – poor appetite, weight loss, urinary frequency but no pneumaturia. • O/E mass in lower abdomen • Hb111, Plts 645, Albumin 28g/l, CRP 122 • CT Scan – mass of small bowel with local perforation and fistulation into bladder and sigmoid WHAT NEXT ?
KH 38 female nurse OPTIONS • Medical therapy - ? Infliximab • Resection • Laparoscopic / Laparotomy • Defunction or not ?
KH 38 female nurse LAPAROTOMY 7.11.03 • 20cm mass of fistulating small bowel Crohns • fistulation into dome of the bladder • multiple complex openings into sigmoid over 8cm WHAT NEXT ?
KH 38 female nurse LAPAROTOMY 7.11.03 • ileocaecectomy • broken off dome of the bladder – catheter 10 days • sigmoid cannot be repaired, extensive indurated defect WHAT NEXT ?
KH 38 female nurse LAPAROTOMY 7.11.03 • sigmoid resection, on table lavage and left colo-colonic anastomosis in two layers maxon • end ileostomy and ascending colon mucous fistula
KH 38 female nurse POSTOP. • developed heparin induced thrombocytopenia • LOS 25 days • HISTOLOGY
KH 38 female nurse Crohns disease – small bowel adenocarcinoma arising from dysplastic epithelium
JH 38 female • 9.3.00 perianal Crohns fistula – seton inserted • 13.9.01inflamed stricture upper rectum • 28.1.02 – white cell scan shows uptake in descending colon and sigmoid • 28.11.02 – acute gynae admission with pelvic pain, ultrasound shows complex solid/cystic mass arising from the right ovary
JH 38 female • 12.11.02 – Gynae Laparotomy • inflammed mass involving the sigmoid and the uterus and adenexae. Small amount of pus – colon normal to proximal descending then very abrnormal and thickened.
JH 38 female • sigmoid separated from the uterus and pelvis washed out. • not clear if PID or Crohns so no resection - proximal loop ileostomy brought out. • home pod 17
JH 38 female • gradually improved little in the way of symptoms – attended OPD to reassess pelvis and explore options for re-anastomosis • 24.9.03 – CT showed bilateral adnexal fluid collections • 27.10.03 – Colonoscopy halted at ulcerated mid-rectal stricture • 19.2.04 contrast enema
JH 38 female WHAT NEXT ?
JH 38 female LAPAROTOMY 10.3.05 • TAH and BSO • Left Hemicolectomy – small abscess around very abnormal proximal rectum, so rectum divided at the pelvic floor. • TV colon to distal rectum cross stapled anstomosis • loop ileostomy maintained
JH 38 female POSTOP • initially good recovery • then unwell, low grade pyrexia, superficial wound breakdown • CT presacral fluid collection – small amount of contrast in a 2cm cavity adjacent to anstomosis.