Download
1 / 26
310 likes | 730 Views
Seizures and Status Epilepticus and Non Convulsive Status. Paul Jones PGY3 April 10 2014. Seizure. A seizure is an episode of abnormal neurologic function caused by inappropriate electrical discharge of brain neurons.

E N D
Seizures and Status Epilepticus and Non Convulsive Status Paul Jones PGY3 April 10 2014
Seizure • A seizure is an episode of abnormal neurologic function caused by inappropriate electrical discharge of brain neurons. • Seizures are inhibited by GABA ( ϒ-aminobutyric acid) and failure of this inhibition facilitates seizure spread
Seizure Classification http://www.epilepsy.org.au/about-epilepsy/understanding-epilepsy/seizure-types-classification
Case # 1 • 27 year old female wakes with strange feeling down the right side of her body. She describes it as electrical jolts. She does not notice any abnormal movements. Her husband states she has not had any loss of consciousness. • Vitals: T 37oC; HR 70; BP 93/50; RR 15; SPO2 98%
Case # 2 • 58 year old male witnessed seizure in shopping mall. Evidence of tongue bite and urinary incontinence. Now postictal. • Vitals: T: 37oC; HR 100; BP 141/68; RR 16; Sat 96%
Case #3 • 28 day old female, brought in by parents. Noticed repetitive jerking motion in arm and leg lasting ~5 minutes just after feeding. Now drowsy. Born full term. No complications. SVD. GBS -. • ED vitals: T 36.7; HR 160; BP / ; RR 50
Case #4 • 2 year old male is brought in by his father after having a seizure lasting <5 minutes at home. Initial ED vitals are: • T 38.6; HR 110;BP / ; RR 30; SPO2 98%
Causes of Secondary Seizure Trauma (recent/remote) Intracranial Hemorrhage Structural CNS Abnormalities Infection Metabolic disturbances Toxins or drugs Eclampsia Hypertensive encephalopathy Anoxic-ischemic injury
Doctor I smell burnt toast… Olfactory and gustatory hallucinations may arise from the medial temporal lobes. Visual symptoms such as flashing lights often result from an occipital focus.
Nonconvulsive status epilepticus Characterized by coma, fluctuating mental status, or confusion with minimal or imperceptible convulsive activity. It is confirmed by EEG.
Febrile Seizure A generalized tonic-clonicseizure, lasting < 15 minutes with a fever ≥38oC(≥100.4oF) in a child 6 months to 5 years of age that occurs only once in a 24 hours period.
Eclampsia Combination of seizures, hypertension, edema and proteinuria in pregnant women beyond 20 weeks’ gestation or up to 3 weeks post partum.
Neonatal Seizure < 1 month of age. Full septic workup (blood, urine and CSF) as well as IV antibiotics Blood and CSF testing for herpes simplex and treatment with acyclovir Head CT for concerns of nonaccidental trauma, ICH, infarction or mass Consider inborn errors of metabolism (lactate, ammonia, serum amino and urine organic acids)
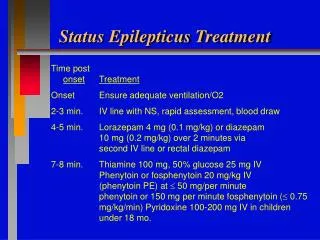
Status Epilepticus Seizure lasting >5 minutes or multiple seizures over a period of >5 minutes. The goal of treatment for status epilepticus is seizure control within 30 minutes of onset.
Approach Airway, Breathing, Circulation IV Access Glucose level Blood pressure, Temperature EKG CBC, Electrolytes Antiepileptic drug level ABG Tox Screen
Tintinalli Dogma? “Lorazepam is the initial agent of choice to control a seizure until more specific agents can be given. IV diazepam is an acceptable alternative.” Tint 7th Ed Cochrane review: No evidence to suggest that intravenous lorazepam should be preferred to diazepam as the first-line drug in treating acute tonic-clonic convulsions including convulsive status epilepticus in children. Some evidence from this review that rectal lorazepam may be more effective and safer than rectal diazepam
Efficacy of Antiepileptics for Status Levetiracetam was 68.5% Phenobarbital 73.6% Phenytoin 50.2%** Valproate 75.7% Lacosamidestudies were excluded from the meta-analysis due to insufficient data.
Case # 1 • 27 year old female wakes with strange feeling down the right side of her body. She describes it as electrical jolts. She does not notice any abnormal movements. Her husband states she has not had any loss of consciousness. • Vitals: T 37oC; HR 70; BP 93/50; RR 15; SPO2 98% • What one investigation would you order? • CT
Case # 2 • 58 year old male witnessed seizure in shopping mall. Evidence of tongue bite and urinary incontinence. Now postictal. • Vitals: T: 37oC; HR 100; BP 141/68; RR 16; Sat 96% • Differential for cause of seizure? • Trauma • ICH • Structural CNS abnormality • Infection • Metabolic • Toxin
Case #3 • 28 day old female, brought in by parents. Noticed repetitive jerking motion in arm and leg lasting ~5 minutes just after feeding. Now drowsy. Born full term. No complications. SVD. GBS -. • ED vitals: T 36.7; HR 160; BP / ; RR 50 • What are four infectious causes of neonatal seizure? • Toxoplasmosis • Rubella • Cytomegalovirus • Herpes
Case #4 • 2 year old male is brought in by his father after having a seizure lasting <5 minutes at home. Initial ED vitals are: • T 38.6; HR 110;BP / ; RR 30; SPO2 98% • What is the incidence of febrile seizures? • 3-5% • What is the risk of recurrence after a single afebrile seizure • Roughly 40% • Lifetime likelihood of seizure is nearly 9%
References • James C. O’Neill. Section 10 Pediatrics. Chapter 78 Seizure and Status Epilepticus in Children. Tintinalli’s Emergency Medicine Just The Facts. • C. Crawford Mechem. Section 16 Neurology. Chapter 147 Seizure and Status Epilepticus. Tintinalli’s Emergency Medicine Just The Facts. • Epilepsy – A Comprehensive Textbook, J. Engle Jr & T.A. Pedley, editors, Lippincott-Raven, 1998 • Chapter 129. Seizures and Status Epilepticus in Children Tintinalli's Emergency Medicine: A Comprehensive Study Guide, 7e, 2011 • Chapter 165. Seizures and Status Epilepticus in Adults Tintinalli's Emergency Medicine: A Comprehensive Study Guide, 7e, 2011 • Cochrane Database Syst Rev. 2002;(4):CD001905. Drug management for acute tonic-clonic convulsions including convulsive status epilepticus in children. Appleton R1, Martland T, Phillips B. • Seizure. 2014 Mar;23(3):167-74. doi: 10.1016/j.seizure.2013.12.007. Epub 2013 Dec 25. The relative effectiveness of five antiepileptic drugs in treatment of benzodiazepine-resistant convulsive status epilepticus: a meta-analysis of published studies. YasiryZ1, Shorvon SD2.