Download
1 / 47
470 likes | 610 Views
Systematically Addressing Health Inequalities in Diabetes Care. The ‘Christmas Tree’ Diagnostic Model National Support Team Health Inequalities. The diagnostic model will support the systematic delivery of the best health outcomes from a given set of interventions.

E N D
Systematically AddressingHealth Inequalities in Diabetes Care The ‘Christmas Tree’ Diagnostic Model National Support Team Health Inequalities
The diagnostic model will support the systematic delivery of the best health outcomes from a given set of interventions. It is based on the assumption that the aim is to achieve optimal health improvement at population level, embracing minimal health inequalities. Commissioning for Best Outcomes Optimal Population Outcome Challenge to Providers Population Focus
This side of the diagram showsaspects of service provision that will influence achievement of best service outcomes from a particular set of interventions Commissioning for Best Outcomes Optimal Population Outcome Challenge to Providers Population Focus 5. Engaging the public 10. Supported self-management 13.Networks,leadership and coordination 9. Responsive Services 4. Accessibility 2. Local Clinical Effectiveness 7. Expressed Demand 6.Known Population Health Needs 1.Known Intervention Efficacy 12. Balanced Service Portfolio 8. Equitable Resourcing 3.Cost Effectiveness 11.Adequate Service Volumes
Optimal Population Outcome 4. Accessibility Services should be based where possible on strong evidence. However, efficacy, based on experimental trials must translate into effective local intervention. This must be constantly checked through local audit and systems of governance. 3.Cost Effectiveness Commissioning for Best Outcomes Challenge to Providers 5. Engaging the public 13. Networks, Leadership and Co-ordination 2. Local Clinical Effectiveness 1.Known Intervention Efficacy
Commissioning for Best Outcomes Challenge to Providers • To have the maximum impact on mortality and morbidity, as many patients with diabetes should be assessed and managed for the following: • Still smoking • Raised BP • Raised cholesterol • Raised HbA1c • possible benefit from low-dose aspirin • Attention should be given to ensuring that patients have been assessed and controlled for all, not just one or two 2. Local Clinical Effectiveness 1.Known Intervention Efficacy
Commissioning for Best Outcomes Challenge to Providers • Are diabetes registers being used to identify potential for multiplicative risk reduction in relation to: • Smoking cessation support? • Alcohol harm reduction? • Physical activity? • Cold/damp housing; fuel poverty in the elderly? • Is there a focus on outcome, rather than • referral; is professional support assertive; is there a menu of support options based on social marketing/insight research? 2. Local Clinical Effectiveness 1.Known Intervention Efficacy
Spearhead PCT where insufficient focus on BP management in patients with Diabetes
Commissioning for Best Outcomes Challenge to Providers Is there a strong focus on performance management of QOF outcomes, with verification sampling where maximum points are claimed, and recovery plans where outcomes are sub-optimal? 2. Local Clinical Effectiveness 1.Known Intervention Efficacy
Commissioning for Best Outcomes Challenge to Providers Is there a diabetes ‘dashboard’ of key information by practice bringing together actual v expected register numbers, QOF outcomes data, prescribing data, and selected hospital admission data, all compared with the district averages (z-score), is seen to be an effective tool for change 2. Local Clinical Effectiveness 1.Known Intervention Efficacy
Commissioning for Best Outcomes Challenge to Providers Are there teams of specialist professionals working in the community to support improved management of diabetes by primary care, maintaining updated manuals, guidelines and protocols; ongoing induction and professional development training; action planning support; evaluation and audit; assistance on procurement , maintenance and effective use of equipment? 2. Local Clinical Effectiveness 1.Known Intervention Efficacy
Commissioning for Best Outcomes Challenge to Providers • Where standards are patchy, best practice engages primary and secondary care together as a compensatory system: • Where primary care cannot offer fully effective care for all patients, this is recognised in a scaled accreditation system eg L1 - L5.Intermediate/ secondary services then provide the missing elements proactively. • All patients can therefore receive effective and comprehensive care. Incentives should support development up the competency scale, which is supported by primary and secondary care practitioners working closely together providing shared care in the community. • The whole system should share responsibility for population level outcomes eg in QOF. This information should be available to all involved. 2. Local Clinical Effectiveness 1.Known Intervention Efficacy
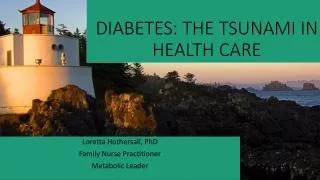
CHD Equity Audit 2006 Selected measures by z scores Example of a good practice 2.5 3.9 4.6 4.3 3.3 2.0 1.5 1.0 0.5 Measures of Need Primary Care Secondary care Tertiary Care 0.0 -0.5 -1.0 Z SCORE -1.5 -2.0 IMD 2004 Outpatients Aspirin Angina Statin Beta Blocker Acute MI ACE Inhibitor CABG/PTCA who smoke % aged 75+ 20% deprived Cardiac CHD Register CHD Register CHD Mortality Heart Failure Standard Ratio Crude Rate % CHD patients A1(a) A1(b) A2 A3 A4(a) A4(b) A4(c) B1 B2 B3 B4 C1 C2 C3 C4 D1 Indicator
Interventions need to be affordable to treat all those who could benefit, and cost beneficial , justifying the opportunity cost against alternative ways to spend 3.Cost Effectiveness Commissioning for Best Outcomes Challenge to Providers 2. Local Clinical Effectiveness 1.Known Intervention Efficacy
Has there been for diabetes, a prescribing cost-versus-QOF outcomes analysis by practice with tailored support to change for poor performers h 3.Cost Effectiveness Commissioning for Best Outcomes Challenge to Providers 2. Local Clinical Effectiveness 1.Known Intervention Efficacy
Bringing services closer to patients and communities may substantially improve uptake, presentation and utilisation. Patient pathways should be designed with this in mind. However, there will possibly be tradeoffs between effectiveness, as interventions are moved away from specialists and specialist facilities, and cost effectiveness if the efficiencies of centralisation are lost. 4. Accessibility 1.Known Intervention Efficacy Commissioning for Best Outcomes Challenge to Providers 2. Local Clinical Effectiveness 3.Cost Effectiveness
5. Engaging the Public Appropriate Utilisaion Delivery systems for interventions should be based around, and directly respond to, the needs and wants of the person, rather than the person having to fit around the needs of the service. Patient and community inputs should be drawn in systematically, not as a tokenistic add-on. Commissioning for Best Outcomes Challenge to Providers 4. Accessibility
Addressing Diabetes Inequalities through Community Engagement Support patient self-management and empowerment, targeting those not achieving treatment goals. Facilitating links to other supports where necessary Raising community awareness of key health messages about prevention/early identification. Case finding and linking to life-style and primary care services Coordination of inputs and output with strategic approach to Community Engagement Outreach to identify reasons for non-engagement with services. Advocacy to improve accessibility of clinical care and ongoing quality of services Improve the skills of primary and specialist care professionals to better meet the needs of patients and make the links to lifestyle change support resources
Challenge to Providers 5. Engaging the Public 10. Supported self-management 9. Responsive Services 4. Accessibility 2. Local Clinical Effectiveness 7. Expressed Demand Attention given to this array of provider-side aspects of delivery should produce good health service outcomes. However, good population health outcomes will not be achieved without also addressing the way communities use the service. 1.Known Intervention Efficacy 6.Known Population Health Needs 8. Equitable Resourcing 3.Cost Effectiveness Commissioning for Best Outcomes Population Focus 13.Networks, Leadership and Coordination
10. Supported Self- Management 13. Networks, Leadership And Co-ordination 9. Responsive Services 7. Expressed Demand It is now possible to get good estimates of health need, either from census, local survey, extrapolation from national surveys or, increasingly, from local clinical systems. Geographical systems can map down to tailored neighbourhoods, census output areas and population quintiles. There are still problems of obtaining good intelligence by ethnicity and other social groupings. 8. Equitable Resourcing Commissioning for Best Outcomes Population Focus 6.Known Population HealthNeeds
Commissioning for Best Outcomes Population Focus • a) Neighbourhood Cluster Types eg: • Older large estates • New estates • Rural and small towns • Ex-Coalfields communities • Mixed young families • Established non-caucasian ethnic • Mobile young • b) Segmentation Groups 6.Known Population Health Needs
One of the major problems of obtaining optimal population health outcomes from service delivery is that people in deprived circumstances often do not present with major health problems until too late. Barriers to presentation include structural issues such as poor access and transport; language and literacy problems; poor knowledge; low expectation of health and health services; fear and denial , and low self esteem. Commissioning for Best Outcomes Population Focus 7. Expressed Demand 6.Known Population Health Needs
Is there a systematic and ongoing strategy to include as many people as possible with established disease onto Diabetes registers? Actual numbers compared to estimates of expected numbers by practice Systematic strategies to ‘sweat the asset’ of practice records to identify patients with disease Variety of ‘segmented’ options to identify patients in the community, scaled up appropriately Commissioning for Best Outcomes Population Focus 7. Expressed Demand 6.Known Population Health Needs
Blackburn with Darwen ThisPCT has been able to to close the register gaps for CVD and Diabetes
NHS Bolton Dr.S.Liversedge
The activity has continued, with the latest figures, for January, continuing the trend. It is estimated that 83-85% of all patients would have been assessed by end March 2009 The figures also show that practices in the more deprived neighbourhoods have been supported to achieve the best results: Deprivation Score No. Practices % Assessed >40 14 79.4 30-39 18 73.7 20-29 12 75.2 <20 11 74.3 It
In order to achieve equitable outcomes for deprived populations, resources applied need , firstly, to be proportionate to need . But they also need disproportionate supplements to reflect the extra effort and support required. 8. Equitable Resourcing Commissioning for Best Outcomes Population Focus 7. Expressed Demand 6.Known Population Health Needs
8. Equitable Resourcing Commissioning for Best Outcomes Population Focus Is there a local mechanism to ‘raise the bar’ beyond QOF maximum for target outcomes, for Diabetes measures. Where extra incentives are used, do they recognise the disproportionate effort/resource to achieve outcomes in disadvantaged elements of the register population ( e.g. using exponential incentives ) 6.Known Population Health Needs
9. Responsive Services When patients do express demand and present for service appropriately, and with resources targeted and available, services should respond actively to channel them effectively to interventions they will benefit from. This should happen regardless of entry point chosen. Patients should receive culturally sensitive help to navigate to relevant service, and should be followed up to ensure arrival and engagement. 6.Known Population Health Needs Commissioning for Best Outcomes Population Focus 7. Expressed Demand 8. Equitable Resourcing
9. Responsive Services Is there a Diabetes QOF Exception Strategy, with clear transparent interpretation of criteria, regular monitoring of outlier levels, and a strongly enforced validation process, including notes audit? 6.Known Population Health Needs Commissioning for Best Outcomes Population Focus 7. Expressed Demand 8. Equitable Resourcing
10 Supported Self-management 7. Expressed Demand 6.Known Population Health Needs Commissioners and providers should ensure that patients are empowered to make informed choices about their treatment, and are educated and supported to utilise treatments and therapies to best effect. This should take into account factors such as literacy, language, culture and IQ. 8. Equitable Resourcing Commissioning for Best Outcomes Population Focus Appropriate Utilisation 9. Responsive Services
Commissioning for Best Outcomes Population Focus 10. Supported Self-management Appropriate Utilisation 9. Responsive Services Is the provision of self-management training scaled-up so as to be able to offer support to all newly diagnosed patients with diabetes? Is there a menu of quality assured options, designed with insight into the preferences of the main range of segmental groups?
Challenge to Providers 5. Engaging the Public 4. Accessibility 2. Local Clinical Effectiveness 7. Expressed Demand Appropriate utilisation of service by the population may require adjustments to supply. 1.Known Intervention Efficacy 6.Known Population Health Needs 3.Cost Effectiveness 8. Equitable Resourcing Commissioning for Best Outcomes Population Focus 10. Supported Self-management Appropriate Utilisation 9. Responsive Services
12. Balanced Service Portfolio Commissioning for Best Outcomes Challenge to Providers Population Focus Capacity of services needs to be commissioned to accommodate appropriate demand while meeting national standards. Service pathways should be balanced to avoid bottlenecks and engineered to allow smooth and efficient progress. 8. Equitable Resourcing 3.Cost Effectiveness 11.Adequate Service Volumes
Workforce planning • Is there PCT support to practices in developing a sustainable workforce, with appropriate skill mix to maintain effective, efficient and affordable register management, recognising the industrial scale of activity • Modelling of person-hours of activity necessary by practice per annum • Modelling of necessary workforce, with skill-mix review • PCT/PBC alliance commissions training eg of NVQ3 Care Technicians, for subsequent employment by practice/practice cluste
6.Known Population Health Needs 1.Known Intervention Efficacy Commissioning for Best Outcomes Challenge to Providers Population Focus 13.Networks,leadership and coordination
Optimal Population Outcome Challenge to Providers 5. Engaging the Public 4. Accessibility 2. Local Clinical Effectiveness 1.Known Intervention Efficacy 12. Balanced Service Portfolio 3.Cost Effectiveness 11.Adequate Service Volumes Commissioning for Best Outcomes = Population Focus 10. Supported Self-management + + + 13. Networks, Leadership and Co-ordination 9. Responsive Services 7. Expressed Demand + 6.Known Population Health Needs 8. Equitable Resourcing