Download
1 / 36
370 likes | 626 Views
Dengue- Blood and Blood Products. Jameela Sathar Hospital Ampang. Haemostatic Changes in Dengue. 1. Vasculopathy/ Endothelial activation - Hess’s test is an early sign - Plasma leakage 2. Thrombocytopenia 3. Coagulation abnormalities. Mitrakul C 1987. DV-ab. DV-ab.

E N D
Dengue- Blood and Blood Products Jameela Sathar Hospital Ampang
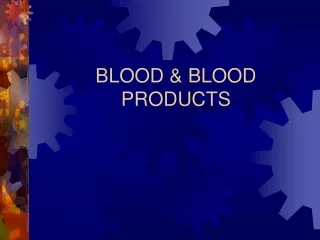
Haemostatic Changes in Dengue 1. Vasculopathy/ Endothelial activation - Hess’s test is an early sign - Plasma leakage 2. Thrombocytopenia 3. Coagulation abnormalities Mitrakul C 1987
DV-ab DV-ab Endothelial activation lumen C C C C IL IL IL EC C Complement: C3a, C5a-C9 Plasma leak Interleukin IL Dengue-infected monocytes
Raised haematocrit • Early evidence of plasma leakage
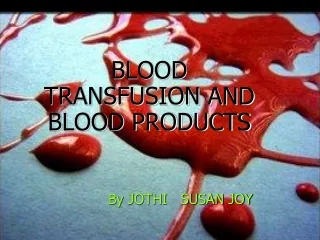
DV-ab DV-ab vWF Platelet activation lumen Plt Plt Plt Plt endothelium
Thrombocytopenia • Platelet count begins to fall towards the end of febrile stage • Lowest during leakage phase • Main mechanism: platelet activation
DV-ab DV-ab VIIa vWF Coagulation activation lumen T Plt T T Plt Plt TF T thrombin fibrinogen
Coagulation Abnormalities Prolonged APTT: 54.6% Prolonged PT: 33.3% Variable but no significant reduction in coagulation factors II, V, VII, VIII, IX, XII and X These do not mean that patient has DIC! Other factors: ? Contact factor deficiency or presence of inhibitor Isarangkura PB 1987
Coagulation Abnormalities • In general, only mild and improves after fluid replacement or cease spontaneously after recovery of illness • However prolonged shock can lead to acidosis and DIC resulting in occult or overt bleeding and end-organ damage
Thrombocytopenia and coagulation abnormalities do not reliably predict bleeding in dengue infection Chaudhary R 2006; Mairahu AT 2003; Krishnamurti C 2001;
Coagulation Abnormalities 48 children with DSS in Vietnam: • Reduced levels of anticoagulant proteins: • PC, PS, AT • Due to plasma leakage and loss • Increased levels of: • Thrombomodulin • Tissue factor • PAI-1 • Due to endothelial activation Wills 2002
Coagulation Abnormalities • Prospective cohort study • 42 Thai children with dengue (20 DF; 22 DHF) • Endothelial cell activation assays were higher in DHF • thrombomodulin • t-PA • TF • ADAMTS • Abnormal vWF multimers were only seen in DHF patients Sosothikul 2007
Increased markers of endothelial activation may promote microvascular thrombosis and end-organ damage Esmon CT 2004
Use blood and blood products with caution and only when indicated
Management of bleeding in dengue • Mild bleeding eg. gums, vagina, epistaxis or petechiae usually cease spontaneously and do not require blood or platelet transfusion • Transfusion of blood and/or blood products in dengue is indicated only when there is evidence of significant bleeding (occult or overt) WHO 1997
Significant occult bleeding • Haematocrit not as high as expected for the degree of shock to be explained by plasma leakage alone • A drop in HCT without clinical improvement despite adequate fluid replacement (40-60 ml/kg) • Severe metabolic acidosis and end-organ dysfunction despite adequate fluid replacement Lum LC 2002
Significant bleeding- which blood products? • Blood transfusion with whole blood or packed cell (preferably less than 1 week old) • ± blood products if in DIC or uncontrolled bleeding
Management of UGIT bleed • Endoscopy and endoscopic injection therapy in upper GIT haemorrhage increases the risk of bleeding and should be avoided • Blood transfusion if significant bleeding Chiu YC 2005
Risk factors for hemorrhage in severe dengueLum et al, J Ped 2002
Risk factors for hemorrhage in severe dengue Lum et al, J Ped 2002
Results • Bleeding is not related to degree of thrombocytopenia • Bleeding is related to the duration of shock due to plasma leakage Lum et al, J Ped 2002
Prevention of hemorrhage in DHF • Early recognition of shock • Prompt correction of shock to prevent acidosis which leads to bleeding
Preventive transfusions in DSS – is it necessary? Lum et al, J Ped, 2003
400 300 Mean % change in platelet count after transfusion 200 100 0 0 1 2 3 4 5 6 7 8 9 10 11 12 Time (hours) after transfusion Behaviour of transfused platelets in DSS Patient no =52 No of transfusions=113 LCS Lum et al, 2003
Life-threatening complications of blood/ blood products • Bacterial contamination • TRALI: Transfusion-related acute lung injury • TTI: Transfusion-transmitted infections • Wrong blood
Infective risks of blood/ blood products (prior to NAT testing)
There is no role for prophylactic transfusion with platelets and fresh frozen plasma in dengue patients
No role for prophylactic transfusion of platelets or FFP • Do not produce sustained changes in the coagulation status and platelet count in patients with DHF/DSS • Do not change or reduce the bleeding outcome in DHF • Inappropriate transfusion of blood products increases the risk of pulmonary oedema and respiratory embarrassment
Adjunctive therapy • Insufficient evidence to support use in dengue of • Recombinant activated factor VII (rFVIIa) in significant bleeding • ivIG • Steroids • The coagulation system is activated in dengue and infusion of activated factor concentrates may increase the risk of thrombosis
Summary • The process of coagulation and platelet activation is an intrinsic part of the disease • Significant bleeding occurs following prolonged shock and acidosis • It is important to recognise and correct hypovolemia to prevent shock which leads to acidosis and DIC/bleeding
Summary • There is evidence that prophylactic platelet transfusion is not useful • There is no role for FFP as a plasma expander • Blood transfusion is indicated if there is evidence of significant bleeding
Pitfalls in the management of DHF • Focus on platelet count instead of hematocrit • Too much focus on bleeding instead of plasma leakage • Too much emphasis on lab results rather than the clinical condition of the patient • Late recognition of shock and inadequate resuscitation
Pitfalls in the management of DHF • Not recognising that Hct does not drop to low levels even in significant bleed • Transfusion of blood only when the Hct falls to a low level may be too late • Too much reliance on platelet and FFP transfusion to control bleeding • Inappropriate and unnecessary transfusion of platelets and FFP will lead to fluid overload