Download
1 / 39
530 likes | 1.73k Views
IBS and the Low FODMAP Diet. Najwa El- Nachef , MD NCSGNA Conference September 20, 2014. Irritable Bowel Syndrome. Affects up to 20% of adults in US Common symptoms include abdominal pain, bloating, constipation and/or diarrhea More frequent among females

E N D
IBS and the Low FODMAP Diet Najwa El-Nachef, MD NCSGNA Conference September 20, 2014
Irritable Bowel Syndrome • Affects up to 20% of adults in US • Common symptoms include abdominal pain, bloating, constipation and/or diarrhea • More frequent among females • Associated with significant decrease in quality of life • Major economic burden on patients, healthcare systems and community • Remains poorly understood Horwitz et al. N Engl J Med 2001;344:1846-50
Mechanism of IBS • Motility • Visceral Hypersensitivity • Central Processing • Genetic Factors • Psychological factors • Inflammation • Gut Microflora • Dietary Factors Lea et al. GastroenterolClin North Am 2005;34:247-55
Treatment for IBS • Focus on reduction of symptoms • Pharmaceuticals • Psychological therapy • Fiber • Probiotics/Antibiotics • Dietary and Lifestyle Interventions
Diet and IBS • Relationship between diet and abdominal symptoms is well recognized • From the patient’s perspective, the most frequently perceived cause for symptoms is food intolerance • Up to 50% of patient’s with IBS symptoms worsen after a meal • 60% of patients with IBS believe they have a food allergy Lea et al. GastroenterolClin North Am 2005;34:247-55
Diet and IBS • Dairy Free • Low fat • High Fiber • No coffee/alcohol • Food diary, self-eliminate • Gluten free diet
Fermentable Carbohydrates • Dietary carbohydrates can be classified into sugars, oligosaccharides and polysaccharides based on their degree of polymerisation. • “Fermentable” owing to their availability for fermentation in the colon, which is either due to the absence or reduced concentration of suitable hydrolase enzymes for digestion or in the case of monosaccharides because of incomplete absorption in the small intestine.
Low FODMAP Diet • Ingested FODMAPs are poorly absorbed in the small bowel • Small, osmotically active molecules which draw water into the large intestine • FODMAPs are also fermented by colonic microflora, producing hydrogen and/or methane gas • The increase in fluid and gas leads to diarrhea, bloating, flatulence, abdominal pain, and distension
Low FODMAP Diet • F: Fermentable • O: Oligo- saccharides • D: Di-saccharides • M: Mono-saccharides • A: and • P: Polyols
Fructose • Simple monosaccharide • Found naturally in many fruits. Also a constituent of sucrose and fructans. • Normally absorbed in small intestine by two mechanisms: • GLUT-5 transporter- present throughout small intesine. • GLUT-2 transporter- requires equal amounts of glucose for more effective absorption. • Failure to completely absorb free fructose leads to its delivery in the colon. • Colonic bacteria rapidly ferment free fructose to hydrogen, carbon dioxide and short-chain fatty acids.
Fructans • Major source of fermentable carbohydrates • Minimal digestion due to absence of enzymes in the human GI tract to digest the fructosyl-fructose glycosidic bonds • Wheat and onion are major sources • Commercial fructansdervied from sucrose or chicory root are increasingly added to prepared foods due to their textural and sensory properties
Galacto-oligosaccharides • Humans lack a-galactosidase enzymes, leading to the availability of GOD for colonic fermentation • Milk, legumes and some grains, nuts and seeds
Polyols • Sugar Alcohol • Absorbed in small intestine by passive diffusion • Present in fruits and vegetables • Commonly used in artificial sweeteners (sorbitol, mannitol, xylitol) • Large amounts can cause osmotic diarrhea
Foods to eliminate • Fructans and galactans: wheat and rye in large amounts, onions, garlic, inulin, legumes, lentils, artichoke, soy milk and almond milk • Lactose: milk, yogurt, ice cream, soft cheese • Excess fructose: high fructose corn syrup, honey, agave, and various fruits (such as apple, pear and watermelon) • Polyols: stones fruits (peach, plum, cherry), mushroom, cauliflower and sorbitol/mannitol
Permissible Foods • Grains: rice, oats, gluten free pasta, some gluten free breads and cereals • Fruits: berries (except blackberries), citrus, banana, grapes, honeydew or cantaloupe melon, kiwifruit • Vegetables: Carrots, corn, eggplant, zucchini, peppers, green beans, lettuce, cucumber, potato, and tomato are a few. • Meats: All meats; avoid processed meats that contain ingredients like high fructose corn syrup, milk solids, or onion/garlic powder • Milk: Lactose free milk, rice milk, lactose free yogurt, hard or ripened cheeses like cheddar and feta
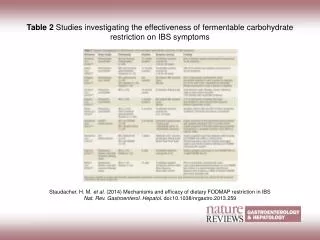
Studies of the mechanisms underlying the effects of fermentable carbohydrates on gastrointestinal symptoms
Delivery of Water/Fermentable Substrate • Ileostomy volunteers • Two diets tested for 4 days each. One high in FODMAPs and one low in FODMAPs • All food prepared by investigators • At baseline and on day 4, 24 hours effluent collected • 10 patients, ileostomy because of IBD, no active disease Barrett et al. Aliment PharmacolTher 2010 Apr;31(8):874-82
Main effluent weight significantly less during LFD • Subjects perceived significantly thicker consistency on LFD
MRI Data with and without FODMAPs Murray et al. Am J Gastroenterol 2014;109:110-9
Shepherd 2008 • Double blinded, randomized placebo-controlled rechallenge trial • 25 patients responded to dietary change • Patients were randomly challenged by graded dose introduction of fructose, fructans or glucose taken as drinks • 70-80% developed symptoms when rechallenged Shepherd. ClinGastroenterolHepatol 2008; 6: 765–71.
Positive Global Symptoms Shepherd ClinGastroenterolHepatol 2008;6:765-771
Low FODMAP Diet v. Standard Dietary Advice Staudacher J Hum Nutr Diet 2011;5:487-95
Halmos 2014 • Crossover trial, 30 patients with IBS and 8 healthy individuals • Randomly assigned to groups that received 21 days either of diet low in FODMAPs or a typical Australian diet • Washout period 21 day before crossing over to the alternate diet. • Almost all food was provided during the interventional diet periods • All stools were collected from days 17-21 and assessed for frequency, weight, water content
“I don’t know what the heck gluten is either but I’m avoiding it- just to be safe.”
Is Gluten the Key Player? Supplementary Figure 1 Recruitment pathway and reasons for screen failure. Recruitment survey was a 23-item questionnaire about symptoms, diet, and investigations for celiac disease described previously.<ce:cross-refrefid="bib20" id="crosref0245"> 20 </c...
Figure 2 Change in symptom severity from run-in for each dietary treatment over 7-day study period. Data shown represent mean ± SEM. Differences across the treatment arms were compared by Friedman test, in which overall symptoms ( P = .001), bloating ( P ... Biesiekiersk Gastroenterology, Volume 145, Issue 2, 2013, 320 - 328.e3 i
FODMAP Popularity • 668,000 results on Google • 16,000“Likes” on Facebook • Several Apps available • Many complain too restrictive
Summary • FODMAPs do not cause IBS • Delivery of dietary FODMAP to the distal small and proximal large intestine is a normal phenomenon, one that will generate symptoms if the underlying bowel response is exaggerated or abnormal.
Summary • Limited data, which are mainly composed of studies with relatively small sample sizes, support IBS symptom improvement with a low-FODMAP diet. • Beneficial effect of a low FODMAP diet does not appear to be predominantly based on gluten avoidance • No definite biomarkers as of now that are associated with symptom response