Multiple Simultaneous Coronary Occlusions in Acute Myocardial Infarction: A Case Report
This case report presents a 44-year-old male smoker, with no other coronary risk factors, who experienced an antero-septal myocardial infarction complicated by thrombus formation in the circumflex coronary artery. Despite early thrombolytic therapy resulting in resolution of ST-segment elevation, the patient developed multistenosis and anterograde dissection requiring stenting. His peak creatine kinase level was 6300 IU, and he was ultimately discharged with appropriate medications. This case highlights the need to consider simultaneous coronary occlusion in acute myocardial infarction presentations.

Multiple Simultaneous Coronary Occlusions in Acute Myocardial Infarction: A Case Report
E N D
Presentation Transcript
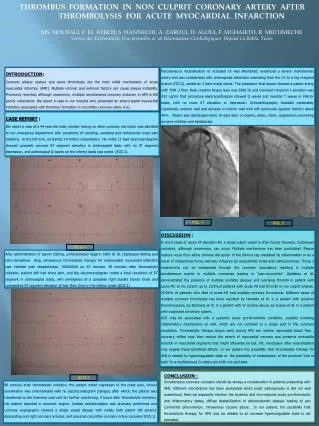
INTRODUCTION: Coronary plaque rupture and acute thrombosis are the main initial mechanisms of acute myocardialinfarction (AMI). Multiple intrinsic and extrinsic factors can cause plaque instability. Previously reported, although uncommon, multiple simultaneous coronary occlusion in AMI is still poorly understood. We report a case in our hospital who presented an antero-septal myocardial infarction associated with thrombus formation in circumflex coronary artery (Cx). Percutaneous recanalization of occluded Cx was attempted, evidenced a severe multistenosis artery and was complicated with anterograde dissection extending from the Cx to a big marginal branch (FIG.2), scaled by 2 bare metal stents. The procedure final aspect showed a patent artery with TIMI 3 flow. Peak creatine kinase level was 6300 IU and maximum troponin I elevation was 432 ng/ml. Post procedure electrocardiogram showed Q waves and inverted T waves in inferior leads, with no more ST elevation or depression. Echocardiography revealed moderately hypokinetic anterior wall and akinesia in inferior wall with left ventricular ejection fraction about 45%. Patient was discharged home 10 days later on aspirin, plavix, statin, angiotensin converting enzyme inhibitor and betablocker. THROMBUS FORMATION IN NON CULPRIT CORONARY ARTERY AFTER THROMBOLYSIS FOR ACUTE MYOCARDIAL INFARCTION MS. MOURALI, F. EL AYECH, S. HANNECHI, A. ZAROUI, H. ALOUI, F. MGHAIETH, R. MECHMECHEService des Explorations Fonctionnelles et de Réanimation Cardiologiques. Hôpital La Rabta. Tunis CASE REPORT : We report a case of a 44-year-old male, smoker having no other coronary risk factor was admitted to our emergency department with symptoms of vomiting, sweating and retrosternal chest pain radiating to the left arm, all started 1H before presentation. His initial 12 lead electrocardiogram showed upwardly concave ST segment elevation in anteroseptal leads with no ST segment depression, and pathological Q waves on the inferior leads was noted (ECG.1). E F FIG. 1 FIG. 2 DISCUSSION : In most cases of acute ST elevation MI, a single culprit vessel is often found. However, multivessel occlusion, although uncommon, can occur. Multiple mechanisms has been postulated. Plaque rupture occur from either primary disruption of the fibrous cap mediated by inflammation or as a result of intraluminal forces extrinsic influence by sympathetic tones and cathecolamines. Those 2 mechanisms can be widespread through the coronary vasculature resulting in multiple simultaneous events in multiple coronaries leading to “pan-coronaritis”. Goldstein et Al. demonstrated the presence of multiple unstable plaques and overlying thrombi in patient with acute MI. In his cohort, up to 32.8%of patients with acute MI had thrombi in non culprit arteries. 25-50% of patients who died of acute MI had multiple coronary thrombosis. Different cases of multiple coronary thrombosis has been reported by Hamada et Al. in a patient with systemic thrombocytosis, by Stenberg et Al. in a patient with IV cocaine abuse, by Suzuki et Al. in a patient with suspected corornary spasm.. ACS may be associated with a systemic acute pro-thrombotic condition, possibly involving inflammatory mechanisms as well, which are not confined to a single spot in the coronary circulation. Thrombolytic therapy begun early during AMI can restore myocardial blood flow , coronary reflow may then reduce the extent of myocardial necrosis and preserve contractile function in myocardial segments that might otherwise be lost. Yet, reocclusion after recanalization may negate these beneficial effects. In our patient the possibility that thrombolytic therapy for AMI is related to hypercoagulable state or the possibility of embolization of the proximal "clot in lysis” to a multistenosis Cx artery are both not excluded. ECG 1 After administration of aspirin 250mg, unfractionated heparin 5000 UI IV, clopidogrel 600mg and nitro-derivatives 6mg, intravenous thrombolytic therapy for anteroseptal myocardial infarction was initiated with streptokinase, 1500000UI on 45 minutes.30 minutes after thrombolytic initiation, patient still had chest pain, and the electrocardiogram noted a total resolution of ST segment in anteroseptal leads, with emergence of a complete right bundle branch block and unexpected ST segment elevation of less than 2mm in the inferior leads (ECG.2). CONCLUSION : Simultaneous coronary occlusion should be always a consideration in patients presenting with AMI. Different mechanisms has been postulated which exact pathogenesis is still not well understood. Here we especially mention the systemic and loco-regional acute pro-thrombotic and inflammatory states, diffuse destabilization of atherosclerotic plaques leading to pan coronaritis phenomenon, intravenous cocaine abuse… In our patient, the possibility that thrombolytic therapy for AMI may be related to an increase hypercoagulable state is not excluded. ECG 2 90 minutes after thrombolytic initiation, the patient noted regression of the chest pain, clinical examination was unremarkable with no electrocardiogram changes, after which, the patient was transferred to the intensive care unit for further monitoring. 4 hours after thrombolytic initiation, the patient reported a recurrent angina. Cardiac catheterization was promptly performed and coronary angiography showed a single vessel disease with widely both patent left anterior descending and right coronary arteries, and proximal circumflex coronary artery occlusion (FIG.1).