Cricoid Force in Children: Analysis and Application
Learn about the necessary cricoid forces in children, practical application, and comparison with adult values to prevent airway issues during medical procedures.

Cricoid Force in Children: Analysis and Application
E N D
Presentation Transcript
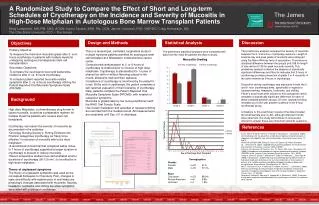
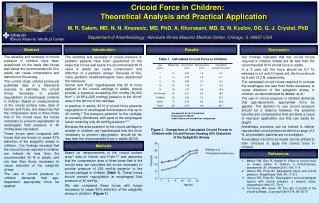
Cricoid Force in Children: Theoretical Analysis and Practical ApplicationM. R. Salem, MD, N. N. Knezevic, MD, PhD, A. Khorasani, MD, G. N. Kozlov, DO, G. J. Crystal, PhDDepartment of Anesthesiology, Advocate Illinois Masonic Medical Center, Chicago, IL 60657 USA Abstract Results Introduction Discussion The reliability and necessity of cricoid pressure in children have been questioned on the basis that forces well below the recommended 30 N in adults can cause compression and distortion of the airway. The current study utilized previously published data in a theoretical exercise to estimate the cricoid forces necessary to prevent regurgitation of esophageal contents in children. Based on measurements of the cricoid surface area, data of Vanner and Pryle, and assuming that the compression area is three times that of the cricoid area, the forces necessary to prevent regurgitation at esophageal fluid pressure of 40 mmHg were calculated. These forces were compared with forces that are known to cause 50% distortion of the subglottic airway in children. Our findings revealed that the cricoid forces required in children are indeed far less than the recommended 30 N in adults, and are less than those necessary to cause distortion of the subglottic airway. The use of cricoid pressure in children demands that age-dependent appropriate force be applied. The reliability and necessity of cricoid pressure in pediatric patients have been questioned on the basis that forces well below the recommended 30 N value in adults can cause compression and distortion of a pediatric airway.1 Because of this, many pediatric anesthesiologists have abandoned the maneuver. Vanner and Pryle2 hypothesized that 30 N force applied to the cricoid cartilage in adults, should provide a pressure exceeding 200 mmHg [30,000 N/m2 = 30 KPa (225 mmHg)] posterior to the 10cm2 area of the lamina of the cartilage. In practice, in adults, 30 N of cricoid force prevents regurgitation of esophageal fluid pressure only up to 40 mmHg.3 The pressure posterior to the cartilage is unevenly distributed, with parts of the esophageal lumen receiving only 40 mmHg pressure.2,3 Because the area posterior to the cricoid cartilage is smaller in children, we hypothesized that the force necessary to prevent regurgitation, should be far less than the recommended force in adults (30 N). Our findings indicated that the cricoid forces required in children indeed are far less than the recommended 30 N cricoid force in adults. In a 3 year old, the force should be 6.7 N, whereas in a 5 and 10 years old, the force should be 8 and 12.2 N, respectively. The calculated cricoid forces required to occlude the esophagus are less than those necessary to cause distortion of the subglottic airway in children, as demonstrated by Walker at al.1 The use of cricoid pressure in children demands that age-dependent, appropriate force be applied. The decision to use cricoid pressure should be a balance between the potential benefits and complications that are likely a result of improper application, but that can easily be taught. Anesthesia providers can be trained to deliver reproducible cricoid pressures within a range of 2 N, and pediatric patients are no exception. A simulated cricoid force model can be utilized to train clinicians to apply the correct force in children. Table 1. Calculated Cricoid Force in Children *assumed to be 3x Cricoid Area #calculated as 3N/cm2 &adult values are included for comparison Figure 1. Comparison of Calculated Cricoid Forces in Children with Cricoid Forces Causing 50% Distortion of the Subglottic Airway Methods References Based on measurements of the cricoid surface area,4 data of Vanner and Pryle,2,3 and assuming that the compression area is three times that of the cricoid area, we calculated the forces necessary to provide pressure of 225 mmHg posterior to the cricoid cartilage in children (Table 1). These forces should prevent regurgitation at esophageal fluid pressure of 40 mmHg. We also compared these forces with forces necessary to cause 50% distortion of the subglottic airway in children1 (Figure 1). • Walker RW, Ravi R, Haylett K. Effect of cricoid force on airway calibre in children: a bronchoscopic assessment. Br J Anaesth 2010; 104: 71-4 • Vanner RG, Pryle BJ. Nasogastric tubes and cricoid pressure. Anaesthesia 1993; 48: 1112-3 • Vanner RG, Pryle BJ. Regurgitation and oesophageal rupture with cricoid pressure: a cadaver study. Anaesthesia 1992; 47: 732-5 • Too-Chung MA, Green JR. The rate of growth of the cricoid cartilage. J Laryngol Otol 1974; 88: 65-70