Download
1 / 12
120 likes | 217 Views
% Survival by Gestational Age and Combined 2006/7, 2008/9 , and NICHD (Stoll, Pediatrics 2010). Survival by Gestation 2006-2009: Comparison with NICHD (Stoll et al. 2010). Inborn-Outborn Survival 2006-2009 by Gestational Age: Compared to NICHD (Stoll Pediatrics 2010 ).

E N D
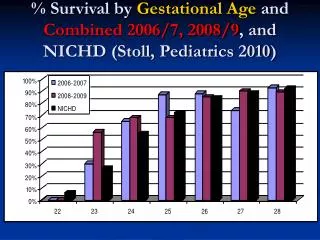
% Survival by Gestational Age and Combined 2006/7, 2008/9, and NICHD (Stoll, Pediatrics 2010)
Survival by Gestation 2006-2009: Comparison with NICHD (Stoll et al. 2010)
Inborn-Outborn Survival 2006-2009 by Gestational Age: Compared to NICHD (Stoll Pediatrics 2010) *NICHD Cohort= 100% Inborn
Inborn-Outborn % Antenatal Steroids 2006-2009 by GA Compared to NICHD (Stoll Pediatrics 2010)
ACOG Committee Opinion, Number 475, February 2011 – Antenatal Corticosteroid Therapy for Fetal Maturation A single course of corticosteroids is recommended for pregnant women between 24 weeks and 34 weeks of gestation who are at risk of preterm delivery within 7 days. A single course of antenatal corticosteroids should be administered to women with premature rupture of membranes before 32 weeks of gestation to reduce the risks of respiratory distress syndrome, perinatal mortality, and other morbidities. The efficacy of corticosteroid use at 32-33 completed weeks of gestation for preterm premature rupture of membranes is unclear, but treatment may be beneficial, particularly if pulmonary immaturity is documented. Sparse data exist on the efficacy of corticosteroid use before fetal age of viability, and such use is not recommended. A single rescue course of antenatal corticosteroids may be considered if the antecedent treatment was given more than 2 weeks prior, the gestational age is less than 32 6/7 weeks, and the women are judged by the clinician to be likely to give birth within the next week. However, regularly scheduled repeat courses or multiple courses (more than two) are not recommended. Further research regarding the risks and benefits, optimal dose, and timing of a single rescue course of steroid treatment is needed.
Inborn-Outborn Cesarean Section Delivery 2006-2009: Comparison to NICHD(Stoll Pediatrics 2010 ) by Gestational Age
Survival by Birthweight 2006-2009: Comparison with NICHD (Fanaroff AJOG 2007) and VON(De Nisi Italian Journal of Pediatrics 2009) *NICHD Cohort= 100% Inborn **VON Cohort= 84% Inborn
IVH by Gestational Age 2006-2009: Comparison to NICHD (Stoll Pediatrics 2010) *NICHD Cohort= 100% Inborn
IVH by Birthweight 2006-2009: Comparison to NICHD(Fanaroff AJOG 2007) *NICHD Cohort= 100% Inborn
PVL by Gestational Age 2006-2009: Comparison to NICHD (Stoll Pediatrics 2010)
PVL by Birthweight 2006-2009: Comparison to NICHD(Fanaroff AJOG 2007)