Download
1 / 22
220 likes | 322 Views
Central nervous system. Central nervous system Radiology college Guanghui Yu. DWI. A B. Normal tissue Brown's movement or diffusion Movement of hydrones at random. Cytotoxic edema

E N D
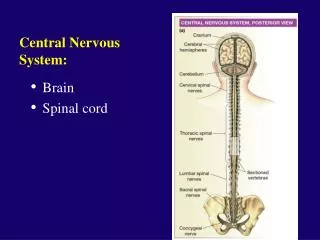
Central nervous system Central nervous system Radiology college Guanghui Yu
DWI A B Normal tissue Brown's movementor diffusion Movement of hydrones at random Cytotoxic edema Brown's movement of hydrones restricted hydrone Cell
Tumor Tumor
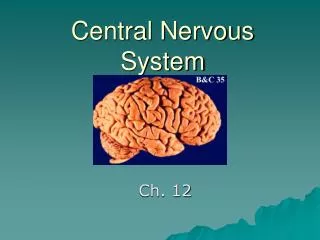
Brain Neoplasm • Neural tissue Neoplasm Neuron permanentcell rare Astrocyte Oligodendrocyte Ependymal cell astrocytoma Glial cell oligodendroglioma ependymoma
Brain Neoplasm Brain Neoplasm • About 80~85% of all intracranial tumors occur in adults • the majority are situated in the supratentorial compartment • the most common intra-axial supratentorial neoplasm is the glioblastoma, while metastasis is the most common intra-axial tumor of the posterior fossa
Brain Neoplasm • Primary cerebral gliomas account for 40~45% of all intracranial tumors • Adult gliomas are mainly supratentorial in location, whereas in children 70~80% are infratentorial • MRI is superior to CT in terms of both tumor detection and delineation • Enhancement after contrast injection is better evaluated by MR owing to its superior sensitivity
Brain Neoplasm Astrocytoma • According to haemorrhage, calcification, edema around tumor, degree of enhancement, astrocytomas are divided into grade I-IV
Brain Neoplasm grade I-II Axial CT without and with intravenous injection of contrast medium. Nonenhancing, hypodense space-occupying lesion infiltrates part of the temporal lobe and insula on the right side. Two arrows indicate the compressed and displaced middle cerebral artery branches within the insular portion of the sylvian cistern
Brain Neoplasm grade I-II axial T2WI. Marked hyperintensity of the tumor due to the high water content of the neoplastic cells. coronal T1WI The tumor is markedly hypointense. Arrowheads point on the right side at the elevated sylvian fissure by the enlarged temporal lobe.
Brain Neoplasm grade I-II axial T2WI Left cerebellar hemispheric pilocytic astrocytoma, partially cystic.The nodular component is isointense. The tumor grows toward the cerebellopontine angle cistern. coronal T1WI. and with isointense nodular components. coronal T1WI following contrast injection. Enhancement of the nodular components
grade III-IV Infiltrating astrocytomas with ill-defined margin
Meningioma • Meningioma arise from specialized meningothelial cells mainly in arachnoid granulations • These tumors mostly affect adults with a strong female predilection (2:1 over males) and are rare in childhood • Gross pathology shows two basic configurations: an oval or lobulated mass with a broad-based attachment to the dura ; or a flattened, linear lesion extending along the dura • Several factors produce tumor heterogeneity: tumoral vascularity, cystic foci and calcifications
Ninety percent are supratentorial • frequently cause hyperostosis of the inner table and can extensively penetrate the skull, causing marked thickening of the bone and osteoblastic reaction ;bone erosion is rare • Brain oedema develops in approximately 50% of meningiomas • Their preferential locations are as follows: parasagittal or attached to the sagittal sinus (25%); the convexity (20%); sphenoid wings (15~20%); parasellar (5~10%); olfactory grooves (2~10%) ; Ten percent are infratentorial and arise from the petrous bone in the cerebellopontine angle, the clivus, the tentorium ; Rarely meningiomas are intraventricular, or arise from the optic nerve sheath
CT shows a well marginated oval or lobulated mass, attached to the dura at an obtuse angle. Most lesions are homogeneously hyperdense, some isodense and a few hypodense • Calcifications are diffuse or focal • Marked homogeneous enhancement
MRI • Isointensity on both T1WI and T2WI • Sixty percent of meningiomas have a "dural tail" of enhancement • Marked homogeneous enhancement
Axial T2WI. Frontoparietal extra-axial space-occupying lesion attached to the falx and the dura of the convexity, on the right side, reaching the midline. The paracentral lobule as well as the most cranial portion of the motor and sensory convolutions are compressed. No significant peritumoral oedema
Dural tail MR T1-weighted sagittal image, following intravenous injection of contrast. Marked homogeneous enhancement of the lesion.