Download
1 / 50
500 likes | 518 Views
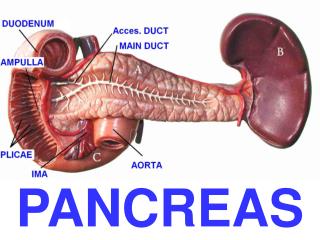
GRADING OF REJECTION IN PANCREAS ALLOGRAFTS Are changes needed?. Cinthia B. Drachenberg, M.D. University of Maryland School of Medicine Baltimore MD. PANCREAS TRANSPLANTATION BACKGROUND. Insulin dependent diabetics (low C-peptide). 13,000 pancreas transplants (1966-99).

E N D
GRADING OF REJECTION IN PANCREAS ALLOGRAFTSAre changes needed? Cinthia B. Drachenberg, M.D. University of Maryland School of Medicine Baltimore MD
PANCREAS TRANSPLANTATIONBACKGROUND • Insulin dependent diabetics (low C-peptide). • 13,000 pancreas transplants (1966-99). • 1200 in the USA in 1998.
PANCREAS TRANSPLANTATIONBACKGROUND • 1y patient survival 95% • 1y pancreas graft function 85% • 1y kidney graft function (SPK) 91% Gruessner and Sutherland in: Clinical Transplants 1999, Cecka and Terasaki Eds. UCLA Immunogenetics Center, Los Angeles CA.
PANCREAS TX NEEDLE BX BACKGROUND • 10 years since Allen et al. described the percutaneous biopsy technique (Transplantation 1991;51:1213). • > 550 done at the Univ. of MD • Complications 2-3%.
PANCREAS TX NEEDLE BX:INDICATIONS • INCREASE IN SERUM AMYLASE/ LIPASE • HYPERGLYCEMIA • UNEXPLAINED FEVER • (DECREASE IN URINARY AMYLASE)
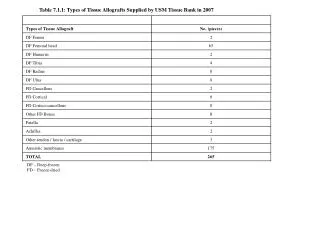
PANCREAS TX NEEDLE BX BACKGROUND • Minimum tissue amount adequate for diagnosis in a needle biopsy: • Two lobules with associated septal tissue (arteries,veins, ducts). • H&E stained sections x3 • Unstained slides
GRADING: ACUTE REJECTION • Acute rejection starts in the septal area with venous endotheliitis. Vessels, acini and ducts are typically involved. (Carpenter et al. Sequential histopathologic changes in pancreaticoduodenal allograft rejection in dogs. Transplantation 1989; 48:764)
GRADING: ACUTE REJECTION 0 No inflammation I Minimal septal inflammation II Venous endotheliitis III Acinar inflammation IV Arterial endotheliitis V Transmural arteritis Drachenberg et al.: Transplantation 1997;63:1579.
GRADING OF REJECTION IN PANCREAS ALLOGRAFTS Are changes needed?
Are changes needed? • Grade I is non-specific with equal significance as grade 0. • Simplification of the 5 grade system is desirable. • The findings in pancreas rejection appear to be analogous to rejection Types I, II and III in the kidney.
PROPOSED GRADING SCHEME 0 No inflammation No rejection I Minimal septal infl. II Venous endotheliitis Type IA III Acinar inflammation Type IB IV Arterial endotheliitis Type II V Transmural arteritis Type III
Correlation with response to treatment: 212 bx, 100 pt TYPE # Treated CS CS/AL 0 90 42 39/13 (33%) 4/1(25%) I A 51 47 34 (94%) 13 (85%) B 48 48 10 (80%) 38 (74%) II A 15 14 2 (0%) 12 (78%) III 8 8 - 8 (12.5%)
PANCREAS NEEDLE BIOPSIESDifferential Diagnosis • Acute rejection • Hyperacute rejection • Pancreatitis – peripancreatitis • Ischemia - thrombosis • Viral infections (CMV, EBV-PTLD) • Drug toxicity • Recurrence of autoimmune disease • Chronic rejection
GRADING OF CHRONIC REJECTION IN NEEDLE BIOPSIES • We had previously proposed a 5 point histological grading scheme for the diagnosis of CR in pancreas transplant needle biopsies. (Papadimitriou et al.Trans. Pro. 1999, 31,614)
GRADING OF CHRONIC REJECTION IN NEEDLE BIOPSIES • PROGRESSIVE FIBROSIS. • PROPORTIONAL ACINAR ATROPHY • TRANSPLANT ARTERIOPATHY*
UPDATED CR GRADING SCHEME • CR 0: No fibrosis • CR I: Mild, Septal fibrosis in <30% of core surface. • CR II: Moderate, Fibrosis in 30-60% of core surface. • CR III: Severe, Fibrosis in >60% of core surface. Acinar atrophy is proportional to fibrosis. Transplant arteriopathy depending on sample.
UPDATED CR SCHEME:CLINICAL CORRELATION The average time from Bx to graft failure per grade: • CR 0: 41 months • CRI: 22.3 months • CII: 10.8 months • CIII: 1.2 m (p=.0001).
UPDATED CR SCHEME:REPRODUCIBILITY 130 biopsies (Bx) from 36 randomly selected patients were analyzed blindly by 3 pathologists • CR 0: k=.94 (p.0001) • CRI: k=.79 (p.0001) • CII: k=.85 (p.0001) • CIII: k=.94 (p.0001)
UPDATED CR GRADING SCHEME The proposed scheme correlates well with graft outcome and predicts to a large extent the remaining time of graft function. The system is based on easily reproducible criteria.