Download
1 / 60
770 likes | 1.61k Views
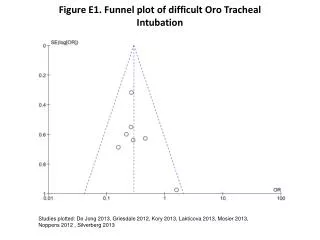
Evaluation and treatment of post intubation tracheal stenosis. Describe 3 qualitative features of post intubation tracheal stenosis Describe 3 diagnostic modalities other than bronchoscopy would you perform to assess the severity, extent and morphology of this patient’s tracheal stenosis?

E N D
Evaluation and treatment of post intubation tracheal stenosis Describe 3 qualitative features of post intubation tracheal stenosis Describe 3 diagnostic modalities other than bronchoscopy would you perform to assess the severity, extent and morphology of this patient’s tracheal stenosis? List 4 therapeutic alternatives for tracheal stenosis Identify 3 airway stricture characteristics that determine the need and type of treatment BI 15. Evaluation and treatment of post intubation tracheal stenosis
Case description An 86 year- old woman with history of stroke and coma requiring prolonged endotracheal intubation and percutaneous dilatational tracheostomy. She was decannulated after several months but required nursing home placement. Now hospitalized with respiratory failure and congestive heart failure (CHF). She was extubated once CHF was treated but within minutes she developed stridor and had to be emergently reintubated. Three days later, she was extubated and then transferred to the regular medicine floor. A few days later, you are consulted for stridor and increased work of breathing. BI 15. Evaluation and treatment of post intubation tracheal stenosis
Case description Medical history includes congestive heart failure, hypothyroidism, hypertension, anemia, dementia and residual hemiplegia from her stroke. Physical examination reveals mild respiratory distress. She follows simple commands and smiles when spoken to. Stridor is present on the tracheal auscultation. Oxygen saturation is 95% on room air. Karnofsky performance score before the episode of respiratory failure was 50 and ASA score at the time of the procedure was 3. Laboratory data are normal She has one daughter who rarely visits her. Nursing home staff say the patient enjoys watching TV and eating. BI 15. Evaluation and treatment of post intubation tracheal stenosis
The Practical Approach Initial Evaluation Procedural Strategies • Examination and, functional status • Significant comorbidities • Support system • Patient preferences and expectations • Indications, contraindications, and results • Team experience • Risk-benefits analysis and therapeutic alternatives • Informed Consent Techniques and Results Long term Management • Anesthesia and peri-operative care • Techniques and instrumentation • Anatomic dangers and other risks • Results and procedure-related complications • Outcome assessment • Follow-up tests and procedures • Referrals • Quality improvement BI #. Evaluation and treatment of post intubation tracheal stenosis
Initial evaluation Chest radiograph revealed “hour glass” configuration of upper tracheal stenosis as well as cardiomegaly and pulmonary vascular congestion. Bronchoscopy showed a triangular severe stomal stricture 3 cm below the vocal cords which during expiration narrowed the tracheal lumen by 100% BI 15. Evaluation and treatment of post intubation tracheal stenosis
Q1: Describe 3 qualitative features of post intubation tracheal stenosis Extrinsic Intraluminal (exophytic, infiltrative, stricture) Mixed Malignant Benign Central Airway Obstruction Qualitative Classification Fixed (simple or complex) Dynamic BI 15. Evaluation and treatment of post intubation tracheal stenosis
Extrinsic, Intraluminal, Mixed Exophytic intraluminal Infiltrative intraluminal Extrinsic Mixed Stricture Inflammatory pseudotumor Thyroid cancer Sarcoma Adenocarcinoma Stricture A B D E C BI #. Evaluation and treatment of post intubation tracheal stenosis
Malignant or Benign Bronchogenic CA Carcinoid LMB Adenoid Cystic LMB A B C BI 15 Evaluation and treatment of post intubation tracheal stenosis
Malignant and Metastatic Bronchogenic Renal Cell Breast Thyroid Colon Sarcoma Melanoma Esophageal Lymphoma Colon Esophageal Melanoma BI 15. Evaluation and treatment of post intubation tracheal stenosis
Benign Stenosis Tracheopathica osteochondroplastica Relapsing polychondritis Post Tuberculosis Wegener’s Granulomatosis Saber-sheath trachea BI #. Evaluation and treatment of post intubation tracheal stenosis Sarcoidosis
More benign tracheal stenosis Idiopathic- isolated ( 59%) GERD Young women age 30-45 Secondary Post intubation(27%) Post tracheostomy ( 11%) Inflammatory diseases Wegener’s Granulomatosis, RP, UC Rheumatoid Arthritis, Sarcoidosis, amyloidosis Post surgical (end-end anastomosis) Post infectious: TB, histo, diphteria, bacterial GERD ( 14%) • Ashiku SK, Kuzuku A, Grillo HC, et al. Idiopathic laryngotracheal stenosis: effective • definitive treatment with laryngotracheal resection. J Thorac Cardiovasc Surg 2004;127:99 –107 • Ann Otol Rhinol Laryngol. 2001 Jul;110(7 Pt 1):606-12 • Otolaryngology–Head and Neck Surgery (2006) 135, 434-437 BI 15. Evaluation and treatment of post intubation tracheal stenosis
Examples of benign tracheal stenosis Chronic post-infectious Post tracheostomy Post-surgical Idiopathic subglottic BI 15. Evaluation and treatment of post intubation tracheal stenosis
Qualitative Classification Of Central Airway Obstruction Extrinsic Intraluminal (exophytic, infiltrative, stricture) Mixed Malignant Benign Central Airway Obstruction Qualitative Classification Fixed (simple or complex) Dynamic BI 15. Evaluation and treatment of post intubation tracheal stenosis
Fixed or Dynamic Fixed Dynamic inspiration expiration Subglottic Stenosis Saber sheath type of tracheomalacia BI 15. Evaluation and treatment of post intubation tracheal stenosis
This is our patient Severe triangular stomal stricture Diagnostic Bronchoscopy video available in the Video Archive Practical Approach to fixed CAO video 1 BI 15. Evaluation and treatment of post intubation tracheal stenosis
So, our patient has a stricture that can be classified … Benign, fixed simple, intraluminal Benign, fixed complex intraluminal Benign, dynamic, complex, extrinsic Benign, fixed, complex, extrinsic Benign, dynamic, simple, intraluminal
Our patient has… Fixed Complex Benign Intraluminal stricture There is limitation to flow both during inspiration and during expiration which makes this lesion fixed; however, any intrathoracic obstruction is made worse by expiration as seen in this case It is complex because of the cartilaginous collapse BI 15. Evaluation and treatment of post intubation tracheal stenosis
Q2. What diagnostic modalities other than bronchoscopy would you perform to assess the severity, extent and morphology of this patient’s tracheal stenosis? Single slice CT scanning 3D internal reformation CT (virtual bronchoscopy) 3D external reformation CT ( virtual bronchography) Magnetic resonance imaging There are no alternatives BI 15. Evaluation and treatment of post intubation tracheal stenosis
3D internal and external reformation CT scanning Advantages Evaluate airways distal to stenosis Plan therapeutic interventions Follow up known conditions; Rule out stent complications Evaluation of conditions where no tissue dx is needed • Disadvantages • Does not allow for the endoluminal visualization of the tracheobronchial tree or • Does not allow for therapeutic and diagnostic maneuvers, such as obtaining culture and biopsy specimens or removing foreign bodies • Radiation risks BI 15. Evaluation and treatment of post intubation tracheal stenosis
External 3D Rendering: Virtual Bronchography Airway stenoses N= 47; TB stenoses 3D: supplemental info in 1/3 cases Complex airway abnormalities N= 15 3D: supplemental info in ½ cases Remy-Jardin M, Remy J, Artaud D, et al. Volume rendering of the tracheobronchial tree: clinical evaluation of bronchographic images. Radiology 1998; 208:761–770 BI 15. Evaluation and treatment of post intubation tracheal stenosis
A statistically significant correlation was found between VB and FB scores (p < 0.0001, r 0.76) VB scores and PFT (p 0.03, r 0.45). Internal 3D Rendering: Virtual Bronchoscopy (VB) Shitrit, D. et al. Chest 2005;128:3545-3550 BI 15. Evaluation and treatment of post intubation tracheal stenosis
Other alternatives MRI small case series support its use for quantifying the degree of airway stenosis Its main advantage is that radiation is avoided Single slice CT scanning may miss focal, short stenoses Normal Stricture BI 15. Evaluation and treatment of post intubation tracheal stenosis
Q3: List 4 therapeutic alternatives for fixed tracheal stenosis Tracheal sleeve resection Radial incision and dilation Airway stent insertion Tracheostomy BI 15. Evaluation and treatment of post intubation tracheal stenosis
Tracheal stenosis 1: Resection and anastomosis Sleeve Resection and reanastomosis ( 90% success rate) Maximum 3-5 cm length; Dehiscence; infection; recurrent laryngeal nerve injury Death ~ 5% Restenosis 8% Mid tracheal repair better than subglottic Courtesy of Charles-Hugo Marquette Clinique des Maladies Respiratoires Centre Hospitalier Universitaire Lille, France Wright CD et al. J Thorac Cardiovasc Surg 2004; 128:731-739 BI 15. Evaluation and treatment of post intubation tracheal stenosis
Surgery in tracheal stenosis Lower tracheal stenosis Cervical incision or sternotomy End-to-end anastomosis • Subglottic stenosis • Cervical approach • Resection cricoid: • anterior arch • Thyroid-cricoid-trachea anastomosis
But high tracheal surgeries have significant complications Experience is important Not all patients should or can be resected Complications include vocal cord dysfunction, recurrent stricture, voice change, infection and dehiscence
Contra-indications to surgery Poor general condition Neurologic Cardiovascular Pulmonary Ongoing inflammation of the stenosis Recent electrocautery or laser treatments Length of stenosis > 6cm Length of normal subglottic area < 1cm Laryngeal involvement
Radial incision Tracheal Stenosis 2: Radial incision and dilation Laser and dilation Web like: 66% cure after first treatment Mehta AC et al. Chest 1993; 104:673-7 Concentric stenoses- more than one treatment If failure: Surgery Removable stent Laser fiber Post dilation BI 15. Evaluation and treatment of post intubation tracheal stenosis
Radial incision and dilation web-like stenosis radial resection semi circumferential resection Courtesy of Charles-Hugo Marquette Clinique des Maladies Respiratoires Centre Hospitalier Universitaire Lille, France BI 15. Evaluation and treatment of post intubation tracheal stenosis
Example of incision and restenosis Notice charring during healing after radial incisions at three sites Simple, web-like stricture Restenosis with granulation
Tracheal Stenosis 3: Airway Stent Insertion Laser, dilation and stent insertion Complex stenoses ( expert opinion) BI 15. Evaluation and treatment of post intubation tracheal stenosis
Results of silicone stents in tracheal stenosis Mucus plugging, granulation tissue formation and stent migration occur in at least 4, 8, and 10 percent of cases, respectively Stent related complications occur more frequently in patients with benign causes of airway obstruction compared to those with malignancies Dumon JF et al. J Bronchol 1996; 3:6-10 Dumon JF. Chest 1990;97:328-332. • Chest. 1999; 115:532-5. BI 15. Evaluation and treatment of post intubation tracheal stenosis
Stent related adverse effects Mucus plugging Granulation Migration BI 15. Evaluation and treatment of post intubation tracheal stenosis
Covered metal stents are often effective Fixed upper and mid tracheal obstruction by tracheal Adenoid Cystic Carcinoma. Covered metal stent maintained airway patency for 5 years.
But metal stents are also associated with more complications Metal stents should be avoided in the trachea, especially in case of benign disease. Note recurrent subglottic stricture Note broken metal strut
Surgical Tracheostomy Tracheal Stenosis: 4. Tracheostomy Bronchoscopy-guided Percutaneous tracheostomy De Leyn et al., Eur J Cardio-Thorac 2007:32;412-421 BI 15. Evaluation and treatment of post intubation tracheal stenosis
Late Complications of tracheostomy Tracheostomy-induced Tracheal stenosis occurs in 3 regions In the suprastomal region At the level of the cuff At the stomal site BI 15. Evaluation and treatment of post intubation tracheal stenosis
Incidence of tracheostomy-induced tracheal stenosis True incidence is difficult to determine because of inconsistent follow-up Estimated to occur in 1-2% of all cases De Leyn et al., Eur J Cardio-Thorac 2007:32;412-421 Mean onset is earlier with percutaneous tracheostomy in comparison to open surgical tracheostomy: 5.0 weeks vs. 28.5 weeks (p=0.009) Raghuraman et al., Chest 2005;127:879-885 Symptoms are not present until there is 75% reduction in lumen diameter; stridor usuallly present when lumen is < 5 mm diameter Heffner et al., Chest 1986;90:430-436 BI 15. Evaluation and treatment of post intubation tracheal stenosis
Suprastomal stenoses Severe suprastomal stenosis (> 50% of lumen) noted in 23.8% of percutaneous dilational tracheostomies and 7.3% of surgical tracheostomies Koitschev et al Anaesthesia 2006;61:832-837 Superior level of stenosis located at mean distance of 1.6 cm from vocal cords in percutaneous tracheostomy and at 3.4 cm from cords in surgical cases (p=0.04). Might this be secondary to incorrect needle puncture sites? Remember that subglottic region stenoses are difficult to surgically repair because of presence of recurrent laryngeal nerve and external branch of superior laryngeal nerve Raghuraman et al Chest 2005;127:879-885 BI 15. Evaluation and treatment of post intubation tracheal stenosis
Stenoses at the level of the tracheostomy tube cuff Caused by ischemic mucosal damage when cuff to tracheal wall tension exceeds the mucosa capillary perfusion pressure (usually 20-30 mm Hg) Inflammatory histologic changes occur within 24-48 hours. Incidence has been reduced tenfold after transition to high volume-low pressure cuffs. Intracuff pressures must be closely monitored, maintaining both peak inspiratory and expiratory intracuff pressures below 15 mm Hg (definitely below 25 mm Hg). Heffner et al., Chest 1986;90:430-436 BI 15. Evaluation and treatment of post intubation tracheal stenosis
Stomal strictures These are the majority Due to inadequate tracheal incisions, ongoing stomal infection, or a rigid tube-connecting system generating excess tube motion Risk is high if tracheostomy tube is too large: Size 8 tube with 11mm outer diameter recommended as upper limit for men Size 7 with 10 mm outer diameter for women Heffner et al., Chest 1986;90:430-436 BI 15. Evaluation and treatment of post intubation tracheal stenosis
Tracheal stenosis: Adjuvant Therapy Otolaryngol Head Neck Surg 2004; 131:16-20. N= 47 Endoscopic steroid injection: 18 % vs. 15% NS Topical mitomycin C: 75% vs. 18% P < 0.05 Laryngoscope, 116:1923–1925, 2006 N = 36 5 vs. 24 months Ann Thorac Surg 2008;85:1438–9 N=1 antireflux measures BI 15. Evaluation and treatment of post intubation tracheal stenosis
Proposed anti-reflux regimen to prevent recurrent tracheal stenosis PROTONIX 40 MG BID ZANTAC 150 MG QHS FLOVENT 110MCG 2 PUFFS BID BACTRIM 1 TB SINGLE STRENGTH Q DAY PEAK FLOW MONITOR AND KEEP DIARY DAILY BI 15. Evaluation and treatment of post intubation tracheal stenosis
Q4. Enumerate 3 stricture characteristics that determine the need and type of treatment Functional class Extent Morphology Origin Severity BI 15. Evaluation and treatment of post intubation tracheal stenosis
Flow velocity (V) ΔP= k V² ((R/r)²-1)² Functional Class and Severity Degree of obstruction (r) Stenosis R Clinical signs depend on r Asymptomatic until critical narrowing occurs BI 15. Evaluation and treatment of post intubation tracheal stenosis J Appl Physiol. 2006 Nov 30;
Tracheal Stenosis and Symptoms SI= 75% • Severity • Mild < 50% • Moderate 50-70% • Severe > 70% BI 15. Evaluation and treatment of post intubation tracheal stenosis
Morphometric Bronchoscopy and Symptoms in Tracheal Stenosis CSA normal – CSA stenotic CSA normal • Stenotic Index = Trachea X 100% Abnormal Area (Stricture) SI=54% Normal Area BI 15. Evaluation and treatment of post intubation tracheal stenosis
Functional activity and severity Symptomatic Active life style Asymptomatic Inactive life style SI =53% SI=54% BI #. Evaluation and treatment of post intubation tracheal stenosis