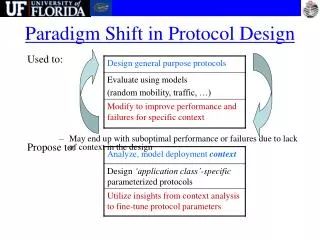
Protocol Design
Protocol Design. Shirley Xu Senior Director QA Shanghai Clinical Research Centre (SCRC) CME Training Course 22 Oct. 2009. Development of a Clinical Trial. Idea Reviews from the experts(Sponsor or CRO) First planning meeting (basic design features)

Protocol Design
E N D
Presentation Transcript
Protocol Design Shirley Xu Senior Director QA Shanghai Clinical Research Centre (SCRC) CME Training Course 22 Oct. 2009
Development of a Clinical Trial Idea Reviews from the experts(Sponsor or CRO) First planning meeting (basic design features) Second planning meeting (draft protocol) Final protocol (ethical and scientific, signed by a statistician) Evaluation (scientific review, IRB, funding) Implementation Final analysis and publication
Evolution of Trial Structure • Large cooperative trials (multicenter trials) • High scientific level protocol • Well-defined administrative structure • Control of performance at all levels (SOPs) • Competent biometric advice (ICH E9) • Careful ethical considerations
Why Multicenter Trials? • Small but important effect • Enhance generalizability of the results • Bring new treatment to the community
Clinical Trial Protocol • A detailed plan giving instructions to the study investigators(doctors) about the way to conduct the study. • Contributors to the protocol development • investigators, • medical personnel from the Sponsor or delegated CRO • representatives from the study monitoring team • project statistician
Crucial Roles of Statisticians • Design (very important!!!) • Monitoring • Analysis • Reporting • New statistical methodology
Sophisticated Statistical Techniques • O’Brien and Fleming Boundaries • Lan & DeMets “Spending function” • Equivalence testing • Repeated measures • Bayesian methods • Nonlinear random effect modeling
Functions of Clinical Trial Protocol • Guideline for the conduct of the trial • Quality control for all aspects of a clinical trial • To provide guidelines to the monitoring groups such as: IEC / IDMC.
Functions of Clinical Trial Protocol • Written agreement between: • the investigator • the participant, • and the scientific community • Legal documents for • FDA and other regulatory bodies • To procure funding
Duration of Protocol Development 7days-6months!!! 4-50 pages long!!!
Three Fundamental Aspects • Which patients are eligible • Which treatment are to be evaluate • How each patient’s response is to be assessed
Background • Rationale • Unpublished work of the investigators • Pharmacological and toxicity • Any new and non standard methods
Specific Objectives • New treatment • New indication • Determine the best of a number of standard treatments • To provide additional data on safety or efficacy
Methods • Hypothesis • Patient population (operational definition) • Inclusion Criteria • Exclusion Criteria More homogeneous less generalizable!!
Treatment Regimens Required procedures for treatment administration, including precise rules for does determinations
Trial Design Control groups • Define and justify the control group • Safety consideration of the placebo group
Trial Design • Randomization (verifiable method) • Method used to generate the allocation schedule • Method of allocation concealment • Packing number • Telephone • Remote data entry • Timing of assignment
Trial Design • Balance on Prognostic Factors • Stratification • Minimization
Trial Design Blinding • Mechanism of treatment blinding • Single, double, triple, quadruple blinding • Assessment of the effectiveness of blinding Experimental design • Parallel designs • Cross-over designs • Factorial designs • Sequential designs
Treatment Phase • Patient management guidelines, including specifications for does reductions, treatment delays and treatment terminations • Schedules of required clinical tests and assessments
Follow-up phase • Schedule of submission of required materials and data, including long-term follow-up • Data and materials submission procedures
Termination • Procedures for ending patients’ participation in the trial
Study Flow Diagram • A flowchart describe how patients progress through the trial • Initial screening • Randomization • Planned schedule • Follow-up visits • Early termination
Outcome Measures • Primary end pointsSecondary end points
Statistical Issues • Power analysis justifying sample size requirements • Interim monitoring and analysis plans • Planned time and methodology of final analyses e.g. ITT, PP, NNT, CI • Methods on secondary aims, compare toxicities
Ethics and Safety • Protection of the trial patient’s right and safety • How the patient is approached for entry into the trial • Regulatory obligations, including informed consent and reporting of adverse events • Plan and action if a SAE be detacted
Other Topics in a Study Protocol • Laboratories • Compliance • How compliance is monitored • Methods used to improve compliance • Organization • Roles • Responsibilities • Budget • Study Forms (CRFs) and data handling • Administrative responsibilities
CRF Design • Identification data • Research data • Administrative data • Regulatory data • Soilker, B. Schoenfelder, J. (1991). Data Collection Forms in Clinical Trials. • Racen Press, New York
Basic Information in CRF • Consent dates • Eligibility checklist • Baseline assessments • Dosing of study medications ( incl. compliance) • Concomitant illness • Safety • Effectiveness • Premature termination of study
Administrative Structure of Multicentre Trials • Steering Committee • Leadership body of the investigative group • Data and Safety Monitoring Committee • Assess the progress, safety and efficacy • Recommendations about continue, modify or terminate.
Study Chairman • Chair steering committee • Responsible for the overall project • Overseeing the design and conduct of the trial • Implementation of SOPs and good clinical practices • Compliance with international and local regulations.
Coordinating Centre • Training • Registration • Randomization • Supplying • Collecting and processing CRFs • Coordination of accrual sites • Auditing study sites • Regulatory reporting
Statistical Centre • Data entry and processing • Ongoing monitoring of toxicity data • Periodical interim analysis of study endpoints • Final data analyses • Preparation abstract and manuscripts
Other Major Personnel • Trial statistician • Clinical research associate • Data manager • Randomization specialist • Quality assurance officer • Computer support personnel • Resource Centre Directors • Training directors • Field site personnel • Independent Data Monitoring Committee
Field Site Personnel • Investigator/Study coordinator • Research Nurse/ • Participants accrual • Intervention • Primary data collection • Follow-up
Standard Operating Procedures (SOPs) • To ensure that the specific tasks in the trial are carried out in a consistent manner. • Topics for SOPs for Investigators:
General Topics • General quality assurance • Quality control procedures • Research personnel qualifications • Clinical audit • Regulatory authority inspections
Ethics • Initial and continuing review by ethics committees • Informed consent • Consent forms and information sheets
Study Setup • Review of: • investigator brochures • Protocols • Protocol amendments • CRFs • agreements (e.g. responsibility, financial, confidential, insurance/indemnity agreement)
Monitoring and Initial Data Review: • Monitoring visits • Source data verification • Data query
Management of Study Medications and Clinical Laboratory Samples: • Shipment • Receipt • Control at study sites • Dispensing inventory • Compliance with use of study medication • Randomization procedures • Clinical laboratory samples
Safety Event Reporting • Definitions • Recording and reporting AEs • Recording and reporting AEs to ethics committees;
Closing The Study • Review of clinical study reports • Premature termination or suspension • Archiving
Some Important ICH Guidelines • E2A Clinical Safety Data Management: Definitions and Standards for Expedited Reporting • E3 Structure and Content of Clinical Study Report (1995) • E6 Good Clinical Practice (1996) • E7 Clinical Trials in Special Populations: Geriatrics (1993) • E8 General Consideration for Clinical Trials (1997) • E9 Statistical Principles for Clinical Trials (1998) • E10 Choice of Control Group in Clinical Trials (TBI) • ICH home page: http://www.ifpma.org/ich1.html • FDA guidelines: http://www.fda.gov/cder/regulatory/default.htm
Federal Office for Human Research Protections (OHRP) • OHRP is responsible for monitoring subject protections at more than 4,000 HHS (Department of Health and Human Services) funded universities, hospitals and other research institutions.
Investigational Melanoma Vaccine Research Study (MV)- Oklahoma Case • OHRP Halts Human Research at University of Oklahoma for Subject Protection Violations • Suspension Date: June 29 2000 • Suspension of 75 federally funded clinical trials performed though the Tulsa campus
Major OHRP Findings: • MV failure to meet GMP • allowed for potential subject exposure to bacterial and viral infections. • 26 of 96 subjects (vaccine arm) died. • Investigators failed to ensure that risks to subjects were minimized.
Major OHRP Findings: • Incomplete informed consent documents • the purpose of the study • Procedures • Foreseeable risks and discomforts • Any expected benefit from study participation • Overstatedthe benefits of the study as capable of preventing the recurrence of melanoma or reducing existing tumor mass • IRB failure to meet its federal regulatory obligations.