Download
1 / 12
120 likes | 202 Views
Frequencies of Resistance-Associated Amino Acid Variants Following Combination Treatment with Boceprevir (BOC) Plus PEGINTRON (PegInterferon Alfa-2b) and Ribavirin (P/R) in Patients With Chronic Hepatitis C (CHC), Genotype 1 (G1).

E N D
Frequencies of Resistance-Associated Amino Acid Variants Following Combination Treatment with Boceprevir (BOC) Plus PEGINTRON (PegInterferon Alfa-2b) and Ribavirin (P/R) in Patients With Chronic Hepatitis C (CHC), Genotype 1 (G1) Richard J.O. Barnard, Lisa D. Pedicone, Eirum Chaudhri, Xiao Tong, Ping Qiu, Clifford A. Brass, Janice K. Albrecht, Patricia Mendez, and Robert Ralston
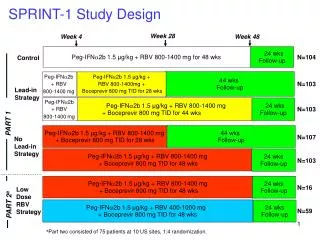
SPRINT-1 Methods Phase 2 study of previously untreated adults with genotype 1 HCV Part 1 - 520 patients randomized to receive Peg-interferon (P)/Ribavirin (R) for 48 weeks (control) or one of four boceprevir regimens – Arms 3 and 5 of Part 1 received a 4 week lead-in with P/R prior to the addition of boceprevir to: Achieve steady state of P/R prior to adding 3rd drug Up-regulate immune response elements Decrease viral load and quasispecies, thereby decreasing resistance Part 2 - 75 patients randomized to receive P/R and low-dose ribavirin
Definitions Sustained Virologic Response (SVR): Plasma HCV-RNA level below the lower limit of detection at follow-up week 12 Incomplete Virologic Response (IVR): A ≥2 log10 increase in HCV-RNA viral load compared with the previous two visits and HCV viral load ≥50,000 IU/mL Viral Breakthrough (BT): Undetectable HCV-RNA and subsequent HCV-RNA ≥2 log10 elevation during therapy Relapse (RL): Undetectable HCV-RNA at end of treatment and detectable HCV‑RNA at follow-up week 24 Nonresponder (NR) (treatment failure): Subjects in Arm 1 with detectable HCV-RNA at treatment week 24 who crossed over to boceprevir Subjects in any of the seven treatment arms with detectable HCV-RNA at end of therapy and at follow-up week 24 Subjects in any of the seven treatment arms with missing HCV-RNA values at follow-up week 24 and do not have an undetectable HCV-RNA at follow-up week 12 Resistance Associated Amino Acid Variant (RAV)
Table 1. Subjects with Baseline RAVs Previously Demonstrated to Confer Reduced Susceptibility to Boceprevir in vitro
Number of Subjects Having RAVs Detected Post-baseline, Including All Patients Treated with Boceprevir 70 60 60 53 50 40 Patients, n 29 30 20 13 11 8 10 5 5 4 3 3 1 1 1 1 1 0 0 0 0 V36I V36L T54A T54S V36A T54C V55A V36G Q41H V158I V36M R155I I170A A156T R155T A156S R155K V158M R155M 17 18 16 13 13 14 12 11 10 Patients, n 8 5 6 4 4 3 2 1 1 1 0 0 0 0 0 0 0 0 0 0 V36I V36L T54A T54S V36A T54C V55A V36G Q41H V158I V36M R155I I170A A156T R155T A156S R155K V158M R155M
Frequency of RAVs for Different Treatment Response Categories Subjects with Variants Detected Subjects with no Variants Detected 80 70 60 50 Patients, n 40 30 20 10 0 IVR BT RL NR IVR = Incomplete Virologic Response, BT = Breakthrough RL = Relapse, NR = Non-responder
RAVs Detected in BOC 28 and 48 Week Treatment Arms Subjects 120 Subjects with RAVs Subjects without RAVs 100 80 Patients, n 60 40 20 0 Arm 2 Arm 3 Arm 4 Arm 5 Arm 6 Arm 7 Lead-in - + - + - -
RAVs Detected with No Lead-in (Arm 2) vs. Lead-in (Arm 3) Study Arms(i.e. Arms where Patients Received a Shorter Duration of Treatment with Boceprevir) 16 14 14 12 12 12 10 8 Patients, n No Lead-in 6 5 5 4 3 3 2 2 2 1 1 1 1 0 0 0 0 0 0 0 0 0 0 0 0 V36I T54C T54A T54S I170T V36L R155I Q41H V158I I170A V55A V36A V36G V36M R155T A156T R155K A156S R155M V158M V36Ipct V36Lpct V36Apct V36Gpct Lead-in
RAVs Detected with No Lead-in (Arms 4) vs. Lead-in (Arm 5) Study Arms (i.e. Arms where Patients Received a Longer Duration of Treatment with Boceprevir) 12 10 10 8 8 7 Patients, n 6 No Lead-in 4 2 2 1 1 1 1 1 1 0 0 0 0 0 0 0 0 0 0 0 V36I V36L T54A T54C T54S V36A V55A V36G I170T V36M Q41H R155I V158I I170A A156T R155K R155T A156S V158M R155M 12 10 8 7 Patients, n 6 5 Lead-in 4 3 2 2 2 1 1 1 1 1 0 0 0 0 0 0 0 0 0 0 0 V36I V36L T54A T54C T54S V36A V55A V36G I170T V36M Q41H R155I V158I I170A A156T R155K R155T A156S V158M R155M
Conclusions In SPRINT-1, combination therapy with boceprevir and peginterferon plus ribavirin increased SVR rates with shorter treatment durations In Non-SVR patients, most frequent RAVs were; Genotype 1a; V36M, T54S, and R155K Genotype 1b; T54A, T54S, A156S, and V170A In subjects with detectable RAVs at baseline, the majority achieved SVR The use of lead-in period led to increased SVR rates and reduced the frequency of T54S variant