Download
1 / 59
600 likes | 803 Views
Learn about pancreatitis, tumors, inherited conditions, and the regulation of pancreatic secretion. Explore the causes, clinical forms, and pathophysiology of acute pancreatitis. Discover the effects of alcohol and food intake.

E N D
DISORDERS OF THE PANCREAS Judit Varkonyi MD.PhD. Med.Habil. 3rd. Department of Internal Medicine. Semmelweis University
General consideration 1/ pancreatitis: a/ acute b/ chronic ● 5ooo new cases/yr in USA ● Still 1o% mortality rate ● 9o% of pancreas tissue has damaged when symptomes of maldigestion (undigested fat, starch and muscle fibers in the stool) appear 2/ tumours: 95% adenocarcinoma ●Signs and symptomes are late manifestations in cancer ……………………………………………………………………… 3/ inherited: cystic fibrosis
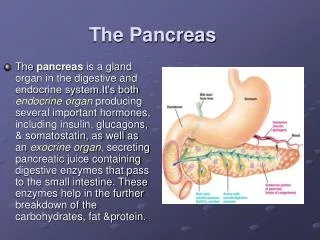
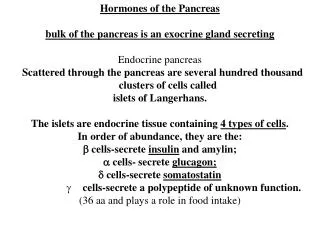
Secreted enzymes • Amylase: hydrolases starch to oligo,- and to disacharides • Lipaze: lipolytic • Proteolytic enzymes: endo,- and exopeptidases ( trypsin,chymotrypsin,etc) • NOTE ! Autodigestion of the pancreas is prevented by the packaging of proteases in precursor forms (zymogens) and by the synthesis of protease inhibitors
Regulation of pancreatic secretion • Pancreatic juice: 1.5-3L/d, basic: ph>8, 2o enzymes • Hormonal and neural regulation Eating → Gastrin →Gastric acid→secretin release →water and electrolyte juice; protein and fat rich food → CCK → enzyme rich fluid secretion • Vagus nerve→gastrin,VIP (secretin agonist) secretion • Regulation at cellular level • Secretin,CCK→acinar cell receptor→ cAMP+cell/membrane changes → enzyme secretion • Exocrine/endocrine relationship: pancreatic glucagon has secretin effect, glucose in large conc. inhibit pancreatic exocrin secretion • Enteropancreatic axis-feedback inhibition: duodenum serin proteases might inhibit pancreatic secretion
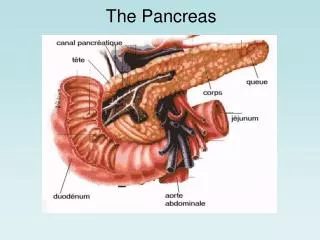
acinar and ductal architecture Efferent duct Centro- Acinar cells and lumen Zymogen granules containig Acinar cells Capillaries Nerve endings
Regulation I. pancreatic duct regulation is under humoral and neuronal regulation • food uptake→gastrin secretion → gastric adic secterion→ Gastric acid entering the duodenum ph≤4.5 → • → Secretin secretion: 2,5 l/d water and bicarbonate rich juice↑ in the ducts • Secretin (duodenum)→ acts through cAMP - K+ és Cl- chanel activation and in the presence of carboanhydrase: the normal function of the Cl- chanels depending on the function of the protein called: cystic fibrosis transmembran conductance regulator (CFTR)
Regulation II. • Cholecystokinin (CCK) (jejunum): one of the main enzime secretion stimulator – by Ach – mediated neuro-hormonal regulation- induced mainly by protein and fat rich food. Inhibited by free trypsin. CCK is the signal of satiety – low level is detected in bulimia nervosa. --------------------------------------------------------------------------- • Gastric emptying induces bowel enterokinase that is activating the trypsinogen-trypsin change. • Trypsin then activates all the other enzymes • Free trypsin left after digestion finished - by negatíve feedback – inhibits further enzyme secterion
PANCREATITIS • Cause: enzymes are activated within the pancreas resulting in autodigestion of cell membranes, with the consequences of oedema, haemorrhage, necrosis in a vitious circle. • Clinical forms, course: • 1. Aute: the inflammation is ending by possible restoration of normal function • 2. Chronic: permanent residual damage
Reasons of acut pancreatitis Iatrogen: ERCP, EST, after heart surgery (Ca, O2↓). Abdominal: penetrating peptic ulcer, abdominal trauma of steering wheel Metabolic: renal insufficiency, diabetic ketoacidosis, hyperparathyreoidism Viral infection: mumps, HBV, Coxakie B, VZ,CMV, Pancreatic cc, Vasculitis: SLE,PAN, Drug induced: eg.furosemid, sulfonamid, NSAID, ACE inhibitors, azathyoprin,…
Clinical features of acute pancreatitis • Abdominal pain (belt like), vomiting and distension ( due to gastric and intestinal hypomotility), tenderness, absent bowel sounds • Tachycardia,BP↓ (hypovolaemia, shock) • Left sided pleural effusion • Cullen’s sign (haemoperitoneum)
Acute pancreatitis pathophysiology • Reason 1/gallstone – increased duct pressure 2/ alcohol - direct toxic 3/ operation: hypoxia, BP dropp--- all resulting: • Az acinar cell damage and consequtive enzyme outflow and premature activation - digesting gland vessel walls causing haemorrhage and cell necrosis. • Necrosis result proinflammatoric cytochin deliberation, granulocyte invasion, vasoactive materials causing increase of vessel wall permeability and by this interstitial oedema. • Impairement of microcirculation by vasoconstriction, capillar stasis, reduced tissue oxigenization, progressive ischaemia further increases vascularis permeability that increase further the extent of the interstitial oedema. microthrombi formation, microinfarcts develop, that eventually result in necrotizating pancreatitis
Effects of alcohol and excessive food intake • Alcohol’s direct cell damage: alcohol- dehydrogenase metabolizing alcohol: the brakedown product acetaldehide is toxic • Alcohol induces viscous, protein rich juice production that increases pressure in the gland by forming protein plugs, • Alcohol induces hyperlipidaemia: >11 mmol/l Tg, fat emboli, fatty infiltartion of acinar cells • Oddi sphincter tone increases
Pathogenesis-enzyme outflow • Lipase→→fat necrosis →calciumsoap formation → hypocalcaemia • Kallikrein→→ oedema,pain,shock • Phospholipase →→ parenchyma necrosis • Elastase→→ vessel wall destruction→ parenchymal bleedings.
Differential diagnosis of acute pancreatitis • 1. perforated peptic ulcer • 2. acute cholecystitis and biliary colic • 3. acute intestinal obstructions • 4.mesenteric vascular occlusion • 5. renal colic • 6. myocardial infarction • 7. dissecting aortic aneurysm • 8. vasculitis (SLE,PAN) • 9. pneumonia • 10. diabetic ketoacidosis
Laboratory findings • Serum, urine amylase, 3-5x normal (↑: 6h,↓: 5d) • Serum lipase (earlier and more prolonged increase↑) • Sebi↑, yGT, SAP, ASAT/ALAT↑ • Leukocytosis, CRP • Hyperglycaemia (insulin↓, glucagon, adrenalin↑) • Trigliceride↑ (reason and cause) • Serum calcium↓ (reason: albumin↓, calcitonin ↑, it is the sign of soap formation)
normális pancreas anatómiai helyzete a körülötte lévõ fontosabb képletekkel (sematikus ábra és UH-os kép)
Ultrahang vizsgálat: A pancreas fejben jelentõs nagyságú, körülírt, közepes echogenitású szolid képlet látható.
CT severity score in acute pancreatitis • A: normal (0) • B: only pancreatic oedema (1) • C: peripancreatic fat involvement (2) • D: one local fluid retention (3) • E: 2-or more local fluid retentions (4) Severity of pancreatic necrosis: A: no necrosis (0) B: 1/3-rd of the gland is involved (2) C: ½ is involved (4) D: more than the half is necrotized (6) ----------------------------------------------------------------------- Severe complication: 3-6 score, severest when 7<
Complications in acute pancreatitis • 1/ pseudocyst formation • 2/ abscess formation (2-3 weeks after the first symptomes, sustained fever/or rapid condition deterioration) • 3/ in haemorrhagic form PCV/HT decreasing • 4/ fistula formation • 5/ Systemic: ARDS,DIC, shock • 6/ transmission to chronic form
Principles of treatment of acute pancreatitis • Hospitalization is required, and in severe cases, therapy should be administered in an intensive care unit. • Intravascular volume • Analgesia • Put pancreas to "rest"Nothing by mouth, nasogastric tube only for ileus or vomiting. Prolonged starvation destruct small intestine- therefore jejunal feeding is to be considerded after a wk if enzymes increase back again while pt starts to eat • Treat complications—pulmonary, shock, renal, metabolic • Remove obstructing gallstone in severe gallstone pancreatitis endoscopically within 36-72 hours • Antibiotics for severe disease
Treatment of acute pancreatitisin 80% selflimited,subsides within 7 days of therapy aim: reducing secretion • 1.analgesics for pain • 2.iv-fluid to maintain volume • 3.no oral alimentation • 4.nasogastric suction to decrease gastrin release • 5.antibiotic therapy of established infection • 6. in fulminant case surgical therapy • 7.in gallstone induced form papillotomy within 36-72h • 8.CT-guided aspiration of pseudocyst and phlegmone • 9.resection of necrotic tissue and drainage • 10.resection of expanding pseudocyst
Endoszkópos sphincterotomia biliaris pancreatitis miattEnélkül:1/ progresszió2/ epekő okozta pancreatitisben a relapsus 50%-ban bekövetkezne 3 hónapon belül
Reasons of Chronicus pancreatitis ALCOHOL: 50-80 g/d consumption (♀,♂) / 10-15yrs
Signs and symptoms of chronic pancreatitis • Chronic abdominal and back painRecurrent attacks of acute pancreatitisPancreatic pseudocyst formationAdult-onset diabetesIntestinal malabsorption and steatorrheaAbnormal liver function testsJaundice from bile duct obstruction
Chronicus pancreatitis pathomechanism • Leading pathogenetic cause: protein plugs or stone in the acinar ducts: multiple ductal obstruction • Increase in intraducatal and acinal pressure • Enzymes pressed out into the interstital space where they became acivated, causing tissue destruction and the vitious circle has begun • The process of acinar atrophy and periductal fibrosis is progressive. Nerve irritation derives pain. Lymphatic vessels also close and therefore clearing of activated enzymes from the interstitial cavity become impossible---enhancing vitious circle. • secondary calcium – cabronate deposition (CALCIFICATION) ↓ ↓ ↓ ↓ ↓ ↓ ↓ ↓ ↓ ↓ ↓ ↓ ↓ ↓ ↓ ↓↓ ↓ ↓ ↓ ↓ ↓ ↓ ↓ ↓ ↓ ↓ ↓ ↓ ↓ ↓ ↓ SYMPTOMES: PAIN, MALDIGESTION: STEATORRHOEA, WEIGHT LOSS
Pancreatic pseudocyst Normal pancreas body and tail Widened, calcificated pancreas head
CT:chronic pancreatitis:diffuse calcification, ductal dilation, gland atrophy, irregular contour, and pseudocysts
Therapy for chronicus pancreatitis • Pancreatic enzymes for the treatment of steatorrhea or pain Enzymes are in use for pain, but all commercially available preparations are of relatively low potency. The potency is reflected in the relative units of lipase per pill. Large numbers of pills must therefore be taken (on average, eight pills with meals and at bedtime). Because these conventional enzymes are destroyed by gastric acid, concomitant therapy with an H2-receptor antagonist or a proton pump inhibitor is usually required. Enteric-coated preparations are the treatment of choice for steatorrhea because they are of much higher potency and do not require suppression of gastric acid.
Therapy for chronic relapsing pancreatitis 1. Diet: alcohol abstinency, protein rich, low fat diet 2. Painkillers: NSAID, nitrate, spasmolytics (epidural). 3. Exocrin (enzime support) és endocrine (insulin) ,H2 block 4. Therapy of complications: • Endoscopic: stop obstruction - EST Drain pancreas pseudocysts by endoscopy alone or US/CT guided by percutaneous drain • Surgery: pseudocyst resection, to solve stenosis
Pancreatic cancer- general considerations • Pancreatic cancer remains one of the most lethal cancers worldwide, with an extremely poor prognosis. This cancer is considered the 5th leading cause of cancer related death. The median survival after diagnosis is generally 2-8 months and five-year survival rate is less than 5% • 8-13/100.000 inhabitants/yr • 50-70 yrs/ Male: smoking, alcohol abuse • Retroperitoneal location therefore insidiously growing, early metastases are the obstacles of eraly diagnosis. • As the diagnosis is often late, surgical therapy almost never mean curative therapy. • Mean survival : 6 mo, after radical surgery: 12-20 mo, 5-yr survival: 1-10% More frequent: • Histologic type: Ductal adenocancer • Location 3x more in the head
Symptomes of pancreatic cancer • Frequent: • abdominal pain ( pressure on ggl.coeliacum) • weight loss • jaundice ( only in pancratic head involvement) • Rare: • IGT • steatorrhoea • Curvoisier sign: palpable painless gallbladder and icterus • migrating thrombophlebitis
Imaging in pancreatic tumours • 1. US: only for tumors bigger than1.5 cm • 2. ERCP: in biliary obstructive jaundice, EST,stent, biopsy • 3. CT: sensitive for tumours smaller than 1.5 cm • 4. MRI: useful in case of iodine allergy and impaired renal function, help in guided biopsy • 5. MRCP: magnetic resonance cholangio- pancreatographia • 6. Endoscopic US in cases of question to identify focal lesions • EUS+FNAB
Endosonographia (EUS) + fine needle aspiration cytology (FNA)
Endosonographia (EUS) + fine needle aspiration cytology (FNA)
CT vs. EUS-FNAB • 185 pts were enrolled whoes ERCP suspected tumour • CT results has been compared to endosonography + FNAB. • Sensitivity • Az EUS + FNAB: 99 % • CT: 57% • Specificity • EUS+FNAB: 92 % • CT: 71 % Harewood GC. és mtsai.: Amer. J. Gastroenterol. 2002;97:1386-91
Pancreatic juice examination • by ERCP pancreatic juice had been collected in 31 patients (12 of them had pancreatic cancer, 11 had chronic pancreatitis and 8 control persons). • K-ras mutation and telomerase activity was determined • A K-ras mutation • cancer 75 % • chr. pancreatitis 27 % • controls 0 % • A telomerase activity • cancer 92 % • chr. pancreatitis 18 % • combining the two method specificity raised to 100 % Myung SJ. És mtsai. Gastrointest. Endosc. 2000;51:708-13