Download
1 / 83
1.18k likes | 2.43k Views
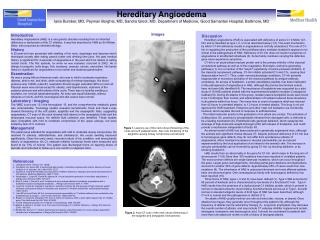
Urticaria and Angioedema. Dr Amir Hossein Siadat. DEFINITION. Urticaria is defined as a skin lesion consisting of a wheal-and-flare reaction in which Iocalized intracutaneous edema (wheal) is surrounded by an area of redness (erythema) that is typically pruritic.

E N D
Urticaria andAngioedema Dr Amir Hossein Siadat
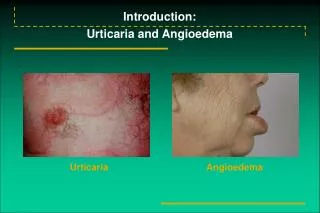
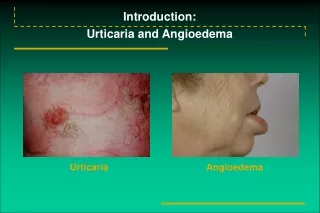
DEFINITION • Urticaria is defined as a skin lesion consisting of a wheal-and-flare reaction in which Iocalized intracutaneous edema (wheal) is surrounded by an area of redness (erythema) that is typically pruritic.
Individual hives can last from as briefly as 30 minutes to as long as 36 hours. • They can be as small as a millimeter or 6 to 8 inches in diameter (giant urticaria). • They blanch with pressure as the dilated blood vessels are compressed, which also accounts for the central pallor of the wheal.
Angioedemas (quinkes edema) affect deeper dermal ,subcutaneus and sub mucosal tissues. • They are usually painfull rather than itchy ,poorly defined and pale or normal in color
Angioedema • Swelling of lips, face, hands, feet, penis or scrotum • Facial swelling most prominent in periorbital area • May be accompanied by swelling of the tongue or pharynx • Larynx virtually never involved
Urticaria is classified to acute and chronic with a time devision between 6w and 3m. • When urticaria is present daily or almost daily for less than 6w it is acute.
CLINICAL CLASSIFICATION OF URTICARIA: • 1)ORDINARY URTICARIA (acute or chronic) • 2)physical and cholinergic • 3)Urticarial vasculitis • 4)Contact Urticaria • 5)angioedema
Up to 50%of patients previously diagnosed as chronic idopathic urticaria have an autoimune bases.
Acute ordinary urticaria may be due to allergy especially in atopics but not in chronic.
ASSOCIATIONS • 1)an association between chronic ordinary u and autoimune thyroid disease • 2)there is a higher frequency of autoimune diseases in patients with autoimune u • The older litrature suggest that chronic idiopathic u may be associated with chhronic infection especially dental and candida of the bowel but now it occures rarely if at all • 4)it has been proposed that H.PYLORI infection may play an indirect role in autoimune chronic u by molecular mimicry in genetically predisposed individuals • 5)no association with malignancies was found in a large study
PREVALANCE: • POINT PREVALANCE=0.1% • Cumulative life time prevalance:0.05-23.6% in general population but a range of 1-5% is more realistic • 72% ordinary urticaria,20%physical and choloinergic,3.4%allergic(exept stings and injected drug),2.1% u.vasculitis,0.5% hereditary angioedema
GENETICS • Hereditary C1 Estrase defficiency angioedema • Muckle Well Syn • Familial cold urticaria • Highly significant linkage of HLA DR4 and HLA DQ8 in chronic ordinary urticaria.
Phathophysiology: • Urticaria is due to a local increase in permeability of capillaries of venules. • It is due to activation of cutaneus mast cells that contain many mediators predominantly histamin.
Pathophysiology of Urticaria Immunologic factors Non-immunologic factors Types II and III complement activation Chemical histamine liberators eg. Opiates, polymyxin antibiotics, thiamine Alternative complement pathway action Physical agents, e.g. cold, heat, sunlight Anaphylatoxins (C3a, C5a) released mediators (particularly histamine) endogenous hormone Cholinergic vasodilating factors Small blood vessel vasodilation Type I IgE mediated genetic factors modulating factors URTICARIA
Clinical features of acute or chronic urticaria: • Ithcing erythematous macules develop into weals consisting of pale to pink edematous raised areas of skin often with a surrounding flare • It occurs any where (scalp and palms),in any number and size, any shape even bulla.
Wheals are often very itchy especially at night and resolve in a few hour without any residue. • Patient always rub not scratch so excoriation is absent. • Sometimes they bruise like in thigh. • Wheals are more prominent at evening and premens
In 50% of of urticaria: there may be angioedema. • Angioedema color is like skin ,most frequently on the face but any other area such as ear ,genitalia,hand and feet • It may last for several days, • It is not always itchy and and may be painful
Urticaria may be proceeded with vomiting. • It may be associated with: • malaise • loss of concentration • feeling hot or cold • headache • vomiting • abdominal pain • diarrhoea • arthralgia • dizziness • scyncope • And even anaphylaxies
Urticaria in infancy: • Cows milk allergy is the commonest etiology of urticaria in infants under 6m • In infants there may be less itching and more tendency to purpuric wheals, • Bizzarly shaped wheals are more common
ACUTE URTICARIA: • 1) Idiopathic: • Most common type: >50% of cases • Sometimes is observed following URTI
2)ALLERGIC: • Is due to interaction of allergen with IgE bound to mast cells • more common in atopics, • Although it is unusual to find an allergic cause, any drug ,food, inhalatant and foreign substance( implants, contactants and injection should be considered).
In an IgE mediated reaction there have been a previous exposure and the reaction will occur in minutes (less than 60 min) • Acute urticaria from drug is common and usually occur within 36h (it is unusual for a drug that is contiuously taken for months
Antibiotics especially penicilin and cephalosporin are common causes. • Risk factors: • previous exposure • reaction to a drug or chemically related drug • intermittant and multiple drug therapy , • familial predisposition
Food: common within minutes but occasionally many hours after due to slow absorption or metabolism • Common food: Shrimp, Crab, Fish, Milk, Nuts, Beans, potatoes, Carrots, Spices, Rice, Banana, Apples, Oranges, • Bee sting allergy usually require multiple exposure but wasp sting allergy is unpredictable
3- None-allergic causes: ASA, NSAIDS, Codein, Morphine, Radiocontast media, Vancomycin,Ciprofloxacin,Polymyxin, Anesthetics can cause histamine release.
Urticaria may follow: EBV, HBV, STREPTOCOCAL THROAT infection in child, Campylobacter
CHRONIC URTICARIA: • 1)Most cases are idiopathic • 2)drugs:mostly attributable to acute type: • Aspirin can aggravate 20-30% of CH.U • The relationship with penicilin is complex and non-confirmed. • ACEIs can cause angioedema or aggravate urticaria
3)reaction to additives in less than10%(tartrazin) • 4)Infection:CH.U is frequently flared by viral infections. • Incidence of bacterial infections such as sinusitis, UTI ,and others are variable, • But if present the treatment of the infection,does not improve urticaria. • H.Pylori, candida and intestinal parasites and toxocara are suggested but not confirmed.
5)Inhalants:Grass,pollens,mould spores,animal danders,house dust and even tobacco smoke are trigger of A or CH U. • If pollen allergy is proven desensitization may be succesfull. • 6)Systemic dis:CVD(SLE and Sjogren),IgM macroglu.
Neither hypo nor hyperthyroidism is commonly associated with CHU,but increased incidence of thyroid autoAb and disturbance of throid function have been reported. • There is no evidence of association with malignancy. • 7)U may worsen premense but if it occures predominantly ,it has been attributed to progestrone sensitivity. • 8)Flare up of U do occur at times of psychological stress.Depression and anxiety were found more frequently in CHU.
DIAGNOSIS • 1)HX taking(onset,duration,and course) • Weals lasting more than 24-48hr particularly if painful or tender suggest the possibility of U.vasculitis or delayed pressure U. • Location, number and shapes of wheals are usually not helpful in most urticarias except for small uniform short lasting weals of cholinergic urticaria or linear lesions of dermatographism . • A family history of atopy ,autoimmunity or angioedema may be useful.
Physical factors should be evaluated. • The presence of angioedema should be noted especially in pharynx or larynx. • Enquire about infection, drug, medication, and food.
INVESTIGATION • 1)Acute U: In patients with life threatening reactions to an allergen ,confirmation is possible with RAST (radioallergosorbent test). • For moderately severe acute reaction, skin prick test may be helpful but is potentially dangerous in a background of anaphylaxis . • 2)Chronic U: history ,specially medications like NSAIDS. • If weals are painful and persist,with present of systemic symptoms ,U vasculitis should be considered.
Allergy to foods is rare,but a food diary may be helpful (time may vary from few second to 24 hr). • Only a CBCdiff ,ESR (SLE,UV,MG), screening test for thyroid autoAB(%14)may be worthwhile. • If angioedema is a major component, screening test for C1 sterase inhibitor deficiency ,should be performed by C4.It is reduced between attacks of angioedema. • If the weals persist for more than 48hr,and not respond to antihistamines a skin biopsy may be helpful.
NATURAL HISTORY • There is no way of predicting the duration of an attack but the severity is often greatest at the onset. • In general spontaneous improvement can occur in%50 within 6months.But %50 of those associated with angioedema can still be expected to have their condition 10 yrs later.
Physical Urticarias May occur so intermittently as to appear acute but typically are chronic entities – most idiopathic Physical Urticarias Symptomatic Dermatographism Cholinergic Cold Induced (Familial or Acquired) Vibratory (angioedema) Pressure – induced, Solar, Aquagenic Physical urticaria
Symptomatic Dermatographism Simply scratching the skin promotes linear hives within minutes Delayed form described Typically is short-lived in duration (1/2 to 3 hours) and responds readily to antihistamines • Symptomatic Dermatographism
Cholinergic Urticaria Goal of raising body temperature (oral) by 0.7oC Hot bath to 420C or having patient exercise Small pruritic papules result surrounded by erythema (but without hypotension) result Passive heat challenge may separate exercise-induced anaphylaxis from cholinergic urticaria Methacholine skin test insensitive (positive result in only 33% of patients with cholinergic urticaria) Cholinergic urticaria
Cold-Induced Urticaria Familial (autosomal dominant) vs acquired (usually infection associated) Acquired form -positive ice-cube challenge Usually responds to cyproheptadine Cold-induced urticaria
Cold Stimulation Time Test (CSTT) Positive in acquired cold-induced urticaria Ice cubes and water in a plastic bag applied to patient’s forearm up to 10 minutes Urticaria results after warming of area Timing of cold stimulus indirectly proportional to severity (less time needed, worse symptoms upon exposure to cold) Many patients with good history for cold-induced urticaria may have negative CSTT Diagnosis of cold-induced urticaria
Delayed Pressure Angioedema ~ 37% incidence of delayed pressure urticaria in chronic urticaria 15 pound weight suspended by thick strap over the shoulder and worn for 15 minutes Typically, erythema with induration and tenderness occurs at least 2 hours after the test
Vibratory angioedema Vortex to induce angioedema in a patient with swelling of hands while driving car Lawlor F et al Br J Dermatol 1989; 120: 93-99