Fetal Chest
360 likes | 630 Views
Fetal Chest. 指導 洪正修主任 楊明智主任 主講 陳志堯醫師. Chest Development Congenital Diaphragmatic Hernia Cystic Adenomatoid Malformation Bronchopulmonary Sequestration. Chest Development Congenital Diaphragmatic Hernia Cystic Adenomatoid Malformation Bronchopulmonary Sequestration.

Fetal Chest
E N D
Presentation Transcript
Fetal Chest 指導 洪正修主任 楊明智主任 主講 陳志堯醫師
Chest Development • Congenital Diaphragmatic Hernia • Cystic Adenomatoid Malformation • Bronchopulmonary Sequestration
Chest Development • Congenital Diaphragmatic Hernia • Cystic Adenomatoid Malformation • Bronchopulmonary Sequestration
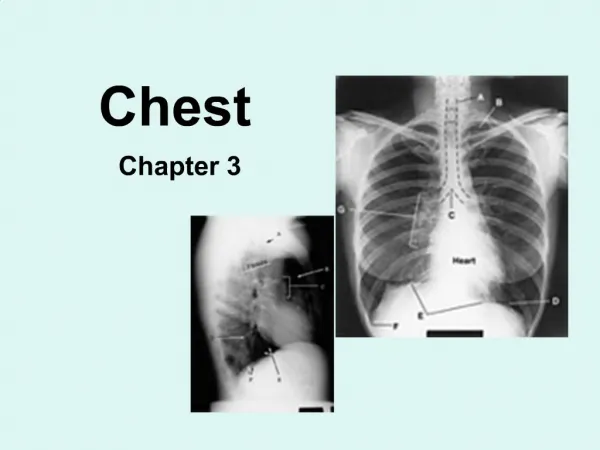
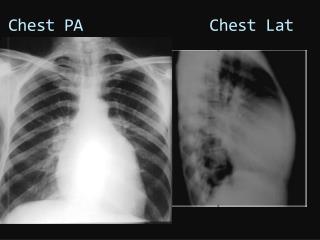
Chest Development (1) • Heart most obvious finding in chest • ¼ to 1/3 of thoracic cavity • Apex direct to left • Cardiac axis approximately 45% • Normal axis excludes significant chest mass • Lungs • Homogenous intermediate echo • Echo G.A • Right side > left side • TC/AC > 0.8
Chest Development (2) • Clinical Importance • Pulmonary hypoplasia:single most important factor determining survival for many conditions. • Oligohydramnios:important etiology component of pulmonary hypoplasia. (oligo as short as 6 days may cause P.H.)
Chest Development • Congenital Diaphragmatic Hernia (CDH) • Cystic Adenomatoid Malformation • Bronchopulmonary Sequestration
CDH • Abnormal AC • Most prenatal diagnosed CDH are large • Hydrops uncommon (unless associated malformations) • Small CDHs are easily missed (ex. stomach not herniated;note cardiac axis)
CDH Left side Right side More difficult May be confused for chest mass Contain liver & intestine (use Doppler showing portal vein) Stomach below diaphragm Gallbladder often herniated • Cystic mass • Absence of fluid-filled stomach • Heart to right • Polyhydramnios • Up to 85% contain herniated liver (liver up) • Use Doppler to follow portal vein (to left)
CDH ~ Pathology • Pulmonary hypoplasia • Up to 50% associated an abnormality • 30% CNS malformation • 20% cardiac anomalies • Renal & spinal • Chromosomal abnormalities common • 16~37% • Trisomy 18,13,21,9 • Epidemiology:1:2000~5000 births • Embryology:failure of fusion of posterior pleuroperitoneal membranes
MRI of CDH (left side)Intestinal loop (red) left lobe of liver (white)
MRI of CDH (right side)RT white:liver,red:stomach LT white:normal right lung,red:intestine
CDH ~ Clinical Issues • 65% survival if isolated • Factors which worsen prognosis • Other abnormalities • Liver in chest (liver up:57% mortality;liver down:7%) • Diagnosed before 24 wks GA • Large size • Right or bilateral • Polyhydramnios • Treatment • In utero repair:not useful • Tracheal occlusion • Postpartum surgery
Chest Development • Congenital Diaphragmatic Hernia (CDH) • Cystic Adenomatoid Malformation • Bronchopulmonary Sequestration
CCAM • Lung hamartoma with proliferation of terminal bronchioles and lack of normal alveoli. • The other classification is based on the size of the cysts • Microcystic (cysts less than 5 mm in diameter) • macrocystic (cysts equal to or greater than 5 mm in diameter) • mixed
CCAM ~ Ultrasonographic Findigs • Best diagnostic clue:solid or cystic lung mass with arterial supply from P.A. • Size:variable,usually contained with one lobe • 95% unilateral and one lobe • Right = Left • May spontaneously regress • Hydrops:most important prognostic factor (< 10%) • Color Doppler:vascular supply from P.A. (D/D with sequestration)
CCAM ~ Image Recommendation • Use Doppler to identify feeding vessels • Monitor closely:every 1~2 wks • Calculate CCAM volume and the ratio to lung
CCAM ~ Pathology • Genetics:sporadic inheritance,no recurrence risk • Most common fetal lung lesion (75%) • Associated anomalies:3~12%
CCAM ~ Clinical Issues • Usually accidently diagnosed • Large for date or polyhydramnios • Prognosis • Majority remain stable or regress in utero • Near 100% mortality with hydrops • Dominant large cyst and CVR > 1.6:indicate poor prognosis (CVR = CCAM vol./HC) • Treatment • None unless hydrops
Chest Development • Congenital Diaphragmatic Hernia (CDH) • Cystic Adenomatoid Malformation • Bronchopulmonary Sequestration (To Be Continued)
For God hath not given us the spirit of fear; but of power, and of love, and of a sound mind.2 Timothy 1:7 Thanks for Listening