Download
1 / 81
950 likes | 1.82k Views
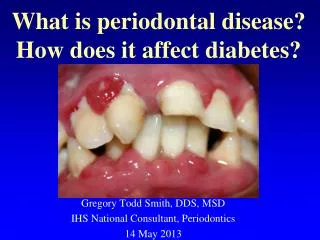
What is periodontal disease? How does it affect diabetes?. Gregory Todd Smith, DDS, MSD IHS National Consultant, Periodontics 14 May 2013. Common infections in the oral cavity. Caries Periapical lesions- nonvital teeth Fungal and viral infections Gingivitis Periodontitis. B Crane 1997.

E N D
What is periodontal disease? How does it affect diabetes? Gregory Todd Smith, DDS, MSD IHS National Consultant, Periodontics 14 May 2013
Common infections in the oral cavity • Caries • Periapical lesions- nonvital teeth • Fungal and viral infections • Gingivitis • Periodontitis B Crane 1997
Gingival polyps/granulomatous tissue Diabetic nonsmoker
Diabetic with mild periodontitis upper arch, moderate periodontitis lower arch.
Oral effects in patients with diabetes: • Increased gingivitis and periodontitis • Caries • Intraoral slow healing • Xerostomia • Burning mouth and tongue • Cheilosis and moniliasis • Multiple periodontal abscesses
Undetected diabetics with severe inflammation and polyps (granulomatous tissue) 23 y.o.
Ulcerated epithelium within infected periodontal pockets allows bacteria, toxins, and inflammatory mediators access to the blood stream. Tooth Gum surface Calculus or tartar Bone Illustration from Scientific American 2006
Moderate periodontitis with moderate to deep pockets and bone loss Estimated 10-20cm2 ulcerated surface and area of tissue necrosis Hujoel 2001
4 cm2 foot ulcer- 3-5X smaller than the ulcerated epithelium within infected periodontal pockets
Infectious diseases can cause changes at distant body sites. “Oral bacteria can explain most, if not all, of the illnesses of mankind.” Miller, 1880 “Focal Infection Theory” in the 1920’s-1940’s. The oral cavity is a portal of entry as well as the site of disease for microbial infections that affect general health status. Surgeon General’s Report on Oral Health in America, 2000 The mouth can become a source of disease or pathological processes affecting other parts of the body…… Surgeon General’s Call to Action to Promote Oral Health, 2003
Periodontitis and Systemic Inflammation • Pro-inflammatory cytokines (IL-1, IL-6, TNF-α) and prostaglandins (PgE2) accumulate in the gum tissues in active periodontitis at extraordinary levels and can enter the circulation. Salvi 1997 • Periodontitis is an anaerobic infection flooding the • blood stream 24 hours a day with endotoxins and • inflammatory mediators. Offenbacher, 1998 • Periodontitis is asso. with increased serum C-Reactive Protein, and periodontal treatment decreases systemic inflammation (CRP, IL-6, TNF- α). Genco 1998, Mattila 2002, Taylor 2006, Marcaccini 2009
Workshop on Inflammation 2008 Experts on inflammation from around the world. Periodontitis is a bacterially induced chronic inflam disease. Inflammatory mechanisms appear to be critical factors in the development and progression of most of the chronic diseases of aging. Periodontitis, DM, CVD, Alzheimer's, Parkinsons, and RA are all interrelated through inflammation. Although our genes do not change, the control of how certain genes are expressed in specific tissues can change substantially throughout our lives by factors such as diet, stress, and bacterial accumulations.
Diabetes and Periodontitis • Epidemiologic Studies in PimasShlossman, Emrich, Knowler, Nelson, Taylor, and others • Diabetics had 3 times greater attachment loss and bone loss than non-diabetics. • Destructive periodontitis occurred much earlier in life in the diabetics (27% of diabetics 15-19 years old). • 11-fold increased risk of progressive bone loss in poorly controlled diabetics. • 15X more likely to lose all their teeth.
Diabetes and periodontitis • A review of 55 studies involving subjects with diabetes found consistent evidence of increased: • Prevalence of periodontitis • Incidence of periodontitis • Severity of periodontitis • Extent of periodontitis • Progression of periodontitis Taylor, CCED 2004 Taylor, Oral Diseases 2008 Dose-response relationship- as glycemic control worsens, periodontitis worsens.
Diabetic Complications: • Atherosclerosis • Microangiopathy • Retinopathy • Nephropathy • Neuropathy • Periodontal Disease
Periodontal destruction in diabetes chemocytosis phagocytosis PMN’s- High glucose Abnormal lipids AGE RAGE Glycation Hyper-responsive monocytes; endothelial cells; fibroblasts; neurons; sm. m. cells Sorbitol IL-1, IL-6, TNF-α, RANKL = Prolonged inflammation collagenase, collagen production oxidative stress and apoptosis Susceptibility to periodontitis
Explain to the patient: White blood cells that fight infection don’t work well. Blood vessels thicken; poor 02 to tissue; allows overgrowth of bacteria that live where there is low 02. Too much tissue destructive enzymes - lose bone and gum attachment to the teeth and gums.
The 2 Way Relationship: Diabetes clearly increases risk for periodontitis. Does periodontitis increase risk for: poorer glycemic control? increased CV and kidney disease? mortality?
Periodontitis aggravates diabetes and its complications Pima study. Taylor et al, JOP 96 Diabetic subjects had an increased risk of a worsening of HbA1c over 2-3 years when severe periodontitis was present at baseline. Findings confirmed of increased risk in Type 2 DMs with severe perio disease. Collins 1998 Patients with IDDM had sig. higher prevalence of proteinurea and cardiovascular complications such as stroke, TIA, angina, and MI when severe perio was present at baseline. Thorstensson J Clin Perio 1996
Periodontal disease is a strong predictor of mortality from ischemic heart disease and diabetic nephropathy in Pimas with type 2 diabetes. Saremi et al, Diabetes Care 2005, n= 628 • Prospective longitudinal study (median 11 years) on the effect of periodontitis on cardiovascular mortality. • After adjusting for many factors, for IHD: • No/mild perio 0 deaths/1000 person-years • Moderate perio 4.8 deaths/1000 person-years • Severe perio 5.7 deaths/1000 person years • For deaths from diabetic nephropathy, there were 0, 0.5, and 5.3 deaths/1000 person-years for no, moderate, and severe perio respectively (p<0.01) (Severe perio = 2.3 X higher risk of cardio mortality 8.5 X higher risk of renal mortality
Effect of periodontitis on overt nephropathy and ESRD in type 2 diabetics. Shultis et al, Diabetes Care 2007 n=529 • Incidence of macroalbuminuria and ESRD increased with severity of periodontitis. • After adjusting for many factors, compared to those periodontally healthy: • Moderate perio OR ESRD 2.3 • Severe perio OR ESRD 3.5 Conclusion: Periodontitis predicts development of overt nephropathy and ESRD in a dose dependent manner in individuals with type 2 DM.
DM and Periodontitis- The 2 Way Relationship DM Poor PMN Function AGE binding/accumulation Inflammatory State Destructive Environment serum lipids blood glucose Further aggravated lipid metabolism & insulin resistance Periodontal Pathogens Increased Periodontal Destruction Chronic infection of periodontitis, with local and systemic inflammation X
The 2 Way Relationship: Can treating the periodontal inflammation and infection improve the diabetic condition?
Periodontal therapy and diabetic control: Recent reviews and meta analyses : • Janket et al JDR 2005Meta analysis of 10 intervention trials. NS but HbA1c decreased 0.7% with abx, 0.4% without. • Darre et al Diabetes Metab 2008 • Meta analysis/Systematic review of 25 studies. SRP provided a small but significant improvement in glycemic control (mean 0.79% decrease). • Teeuw et al Diabetes Care 2010 • Meta analysis/Systematic review. 5 articles met inclusion criteria. Perio tx leads to an improvement of glycemic control in Type 2s for at least 3 months. • Simpson. Cochran Library 2010. Treating perio may lower blood sugar levels in type 2’s. Limited evidence type 1’s.
Diabetic Periodontal Treatment Program Phoenix Indian Medical Center Over 4000 patients with diabetes enrolled since 1998. After periodontal treatment, the patients are placed on 3 to 9 month recalls.
Dental treatment protocol in dms with moderate to severe perio: • Intensive OHI and motivation • 1/2 mouth ultrasonic SRP with LA • Aggressive periodontal pocket debridement in deep pockets. • Extract hopeless teeth • Antibiotic • Doxy 100mg bid X 14 or 21 days • Antimicrobial mouthrinse • Analgesic • Recall 3-6 months
Perio treatment was effective in improving perio health PIMC/ITCA analysis 2010 Over 90% of the patients’ improved or were stabile at their first recall visit from their completion of care visit
Dental Extractions for Periodontal Disease and HbA1c ChangeJeffrey M. Curtis1, Gregory Todd Smith2, Brian A. Grice1, and William C. Knowler11 Phoenix Epidemiology and Clinical Research Branch, NIDDK, NIH, Phoenix AZ2 Phoenix Indian Medical Center, IHS, DHHS, Phoenix, AZ • Type 2 diabetics with severe chronic periodontitis &/or caries received full mouth extractions prior to complete dentures. • Glycated hemoglobins (HbA1c) were obtained by blood draw prior to extractions and 30-200 days post extraction. • Of 87 patients, 30 required at least 4 extractions and received timely HbA1c assays.
HbA1c Change with Dental Extraction HbA1c within 90 days before extraction (closest to extraction date) and 30-200 days after extraction. The change in HbA1c is significant. Mean change is 1.07 percentage points. Median is 0.6 percentage points. Analyses by Dr. Jeff Curtis, NIDDK
There wasno significant change in weight. A1c change was not due to weight loss brought about by inability to eat after extraction or medication change or add’n.
American Diabetes Association’s 1st Symposium on Oral Health with representatives of the American Dental Asso. • Periodontal disease is associated with insulin resistance and poor glycemic control • Systemic inflammation appears to be the critical link between periodontitis and dm. American Diabetes Asso Annual Scientific Session 2008
Medical Guideline on Oral Health for People with Diabetes • Enquire about regular oral health check ups. • Enquire at least annually for symptoms of gum disease, and to seek treatment if present. • Remind that adequate daily oral home care is a normal part of diabetes self-management. • Educate on the relationship between diabetes and gum disease. International Diabetes Federation 2009