Download
1 / 19
190 likes | 338 Views
NOR-MAN RHA. Falls Prevention and Management Program February 2012. Team Members. Team Sponsor: Lois Moberly Executive Director of Clinical services. Darlene Larson Nellie Brown, Joanne Roberts Diane Chambers Kelly Elvin Lori Weiman Pat Kerwin Karen Leifso.

E N D
NOR-MAN RHA Falls Prevention and Management ProgramFebruary 2012
Team Members • Team Sponsor: Lois Moberly Executive Director of Clinical services • Darlene Larson • Nellie Brown, • Joanne Roberts • Diane Chambers • Kelly Elvin • Lori Weiman • Pat Kerwin • Karen Leifso
Purpose of Falls Intervention Team The AIM of this FFLS series is • To provide an interdisciplinary approach to the management of falls • To reduce the number and severity of falls • To develop and deliver education to staff, patients and families on falls prevention and management
STATS • About 40% of older adults who are hospitalized after a fall have suffered hip fractures, and approximately 7% of these result in death1. According to the Canadian Institute for Health Information, falls are the primary cause of injury admissions, accounting for 54.4% of all injury hospitalizations and 75.7% of all in-hospital deaths for clients admitted for injuries2. In total, there were 197,002 hospital injury admissions in Canada with 54.4% caused by falls. • Among Canadians age 65 or older, most injury hospitalizations followed a fall (77% for males, and 88% for females). Those who fall are at higher risk for future falls and injury3. • Identifying patients at risk and implementing falls prevention programs can prevent falls. A 20% reduction in falls would translate to an estimated 7,500 fewer hospitalizations and 1,800 permanently disabled elderly over the age of 65.
FFLS Discussion: • The team approach needs to be a regional approach • New staff orientation- fall management program • The need to develop an audit tool • Find ways to share with staff how program is working • The need for consistent education with nurses • measuring through occurrence reports • We need to start small and trial, if it is successful it will be implemented.
Barriers to FFLS • Time • Staff shortage • New staff • Financial • the inconsistency of staff • not following care plans • also do not measure • No strategy for sustainability.
Intervention Measures There are six measures: • Falls Rate per 1000 Patient/Resident Days (Outcome Measure) • Percentage of Falls Causing Injury (Outcome Measure) • Percentage of Patients/Residents with Completed Falls Risk Assessment on Admission (Process Measure) • Percentage of Patients/Residents with Completed Falls Risk Assessment Following a Fall or Significant Change in Medical Status (Process Measure) • Percentage of “At Risk” Patients/Residents with a Documented Falls Prevention/Injury Reduction Plan (Process Measure) • Restraint Use (Balancing Measure)
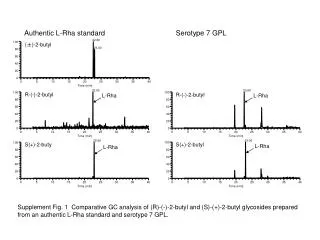
Falls Falls-Acute 2 - Percentage of Falls Causing InjuryMedical Patients
Percentage of Patients with Completed Falls Risk Assessment on AdmissionMedical Patients
Goals • To reduce the risk of falls • To reduce costs of falls • To change attitudes and behaviours by creating a culture of safety
Project NOR-MAN RHA Acute Care December 5 2011PDSA Cycle Reporting Form • What are we trying to accomplish? • Decrease the # of falls • Decrease the severity of injury • Ensure that care plans are specific in regards to identifying triggers and care planning • accordingly • How will we know that a change is an improvement? What will our measurement strategy be? How does this link to our overall measurement and performance monitoring strategies? • Auditing care plans for specificity of interventions • Continue to track and report on the number of falls and the severity of injury • Debrief staff post falls to discuss triggers and possible interventions • What changes can we make that will result in an improvement? How does this PDSA link to other PDSA’s that we have planned?
PDSA Cycle What is our hunch that we that would like to test out? Would documenting more specific interventions result in the reduction of falls and severity injuries? Would developing a new fall risk tool for Patients at risk help staff to investigate interventions and triggers. What do we expect to happen? Reduce falls by 20% Staff will become more engaged and cautious Staff will understand the why’s of falls How will we measure progress? Number of falls Severity of injury related to falls Is this a pragmatic, realistic, learning cycle? Anything else we need to do? Yes we must be consistent in our approach and do a follow up of every fall. We must regularly audit care plans for specificity of interventions.
REQUIRED ORGANIZATIONAL PRACTICE The team implements and evaluates • A fall prevention strategy to minimize the impact of client falls. • The team has implemented a falls prevention strategy. • The strategy identifies the team’s populations at risk of injuries from falls. • The strategy addresses the specific needs of the populations identified. • The team evaluates the falls prevention strategy on an ongoing basis to identify trends, causes and degrees of injury. • The team uses the evaluation information to make improvements to its fall prevention strategy.
What have we did as a organization? • Acute Care Fall Management Program AUGUST 2009 • Falls Self-Learning Package • Tracking system in place
Carry out the plan and document the actions • Revise the Policy • Revise the Morse Fall tool • Revise the Fall Management Prevention Program • Educate every staff
Intervention • Exercise Nurses can use strength training as a component of multi-factorial fall interventions; however, there is insufficient evidence to recommend it as a stand-alone intervention. • Multi-factorialNurses, as part of the multidisciplinary team, implement multi-factorial fall management interventions to prevent future falls. • Medications Nurses, in consultation with the health care team, conduct periodic medication reviews to prevent falls among the elderly in health care settings. Clients taking Antihypertensive, diuretics, laxatives, narcotic analgesics or Psychotropic’s, or more than five medications should be identified as high risk. There is fair evidence that medication review be conducted periodically throughout the institutional stay. • Hip Protectors Nurses could consider the use of hip protectors to reduce hip fractures among those clients considered at high risk of fractures associated with falls; however, there is no evidence to support universal use of hip protectors among the elderly in health care settings. • Vitamin D Nurses provide clients with information on the benefits of vitamin D supplementation in relation to reducing fall risk. In addition, information on dietary, life style, and treatment choice for the prevention of osteoporosis is relevant in relation to reducing the risk of fracture. • Client Education All clients who have been assessed as high risk for falling receive education regarding their risk of falling. • Environment • Nurses include environmental modifications as a component of fall management strategies.