Download
1 / 17
170 likes | 342 Views
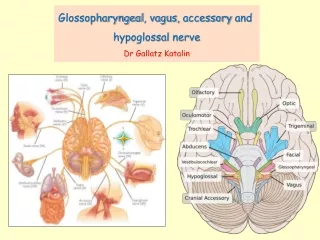
Accessory and Hypoglossal nerves. 11 th CN: Accessory Nerve. Type: Motor (SVE) Origin : 2 roots cranial root : arises from the medulla Spinal root : from upper 5 cervical segments Emerges from : jugular foramen then the 2 roots separate. Cranial Part.

E N D
11th CN: Accessory Nerve • Type:Motor (SVE) • Origin : 2 roots cranial root: arises from the medulla Spinal root : from upper 5 cervical segments • Emerges from : jugular foramen then the 2 roots separate
Cranial Part • Origin:Nucleus ambiguus (NA)in the medulla oblongata • Site of emergence: The fibers emerge from the anterior surface of the medulla oblongata between the olive and the inferior cerebellar peduncle (ICP)
Spinal Part Origin: • Formed by the axons of the nerve cells in the spinal nucleus which is located in the ventral grey horn in the upper 5 cervical segments
The nucleus ambiguus and the spinal nucleus receive bilateralcorticonuclear fibers(from both cerebral hemispheres)
Course • The cranial root : joins the vagus nerve and distributed with its pharyngeal and laryngeal branches • Spinal part: fibers emerge from the spinal cord, form a nerve trunk that ascends into the cranial cavity through the foramen magnum, pass laterally and join the cranial root.
Course • Spinal part ctd.: • Descends first in the carotid sheath (bet. I.C.A. and I.J.V. ) • Then emerges from the sheath, pass backwards, to pierce the sternomastoid m., cross the posterior triangle of the neck to end in the trapezius Supply both muscles Function: • Movements of the soft palate, larynx, pharynx. • Controls the movements of neck
Lesion • Lesion results into: • Difficulty in swallowing and speech • Inability to turn the head • Inability to shrug (raise) the shoulder • Winging of scapula
12th CN: Hypoglossal Nerve Type: Motor (GSE) Origin: Hypoglossal nucleus of the medulla (in the floor of 4th ventricle) Foramen of exit from skull: Hypoglossal canal
The hypoglossal nucleus receives corticonuclear fibers from both cerebral hemispheres EXCEPT the region that supplies genioglossusmuscle (it receives contralateral supply only) Also receives afferent fibers from nucleus solitariusand trigeminal sensory nucleus.
Site of emergence: • The fibers emerge from the anterior surface of the medulla oblongata between the pyramidand the olive. Pyramid Olive
Course • Descends in the carotid sheath between internal jugular vein and internal carotid artery • It leaves the sheath and pass forward and medially crossing ICA &ECA • It enters the digastric triangle • Finally , it pass deep to the mylohyoidmuscle to reach the tongue where it breaks into terminal branches
Course During its initial course, it carries C1 fibers which leave in a branch to take part in the formation of ansacervicalis(a loop of nerves supplying neck muscles) C1 fibers
Supplies motor innervation to all of the muscles of the tongue Except the palatoglossus(which is supplied by the vagus). Carries proprioceptive afferents from the tongue muscles. Distribution: Function: Controls the movements and shape of the tongue during speech and swallowing
LESION Normal • Lesion of the nerve results into: • Loss of tongue movements • Difficulty in chewing and speech • The tongue paralyses, atrophies, becomes shrunken and furrowed on the affected side (LMN paralysis) • On protrusion, tongue deviates to the affected side • If both nerves are damaged, person can’t protrude tongue