Download
1 / 38
380 likes | 577 Views
INCIDENCE OF DELAYS IN CHEMOTHERAPY DUE TO METHOTREXATE TOXICITY IN TREATMENT OF OSTEOSARCOMA. M. Perisoglou, B. Seddon, S. Daniels, N. Mayne, J. Whelan Department of Oncology University College Hospital, London, UK. HIGH-DOSE METHOTREXATE IN TREATMENT OF OSTEOSARCOMA.

E N D
INCIDENCE OF DELAYS IN CHEMOTHERAPY DUE TO METHOTREXATE TOXICITY IN TREATMENT OF OSTEOSARCOMA M. Perisoglou, B. Seddon, S. Daniels, N. Mayne, J. Whelan Department of Oncology University College Hospital, London, UK CTOS, 12th Annual Meeting, Venice 2-4 November 2006
HIGH-DOSE METHOTREXATE IN TREATMENT OF OSTEOSARCOMA • High-dose methotrexate (12 gr/m2): essential component of osteosarcoma treatment CTOS, 12th Annual Meeting, Venice 2-4 November 2006
HIGH-DOSE METHOTREXATE IN TREATMENT OF OSTEOSARCOMA • High-dose methotrexate (12 gr/m2): essential component of osteosarcoma treatment • Supportive measures - iv hydration - urinary alkalinisation - folinic acid rescue (pharmacokinetically guided) CTOS, 12th Annual Meeting, Venice 2-4 November 2006
HIGH-DOSE METHOTREXATE IN TREATMENT OF OSTEOSARCOMA • High-dose methotrexate (12 gr/m2): essential component of osteosarcoma treatment • Supportive measures - iv hydration - urinary alkalinisation - folinic acid rescue (pharmacokinetically guided) • Methotrexate tolerance There is wide intra- and inter-patient variation to MTX tolerance, primary determinant of which appears to be variation in the pharmacokinetics of the drug CTOS, 12th Annual Meeting, Venice 2-4 November 2006
METHOTREXATE TOXICITY • Mucositis / Stomatitis • Bone marrow suppression • Nephrotoxicity • Hepatotoxicity • Dermatitis • Encephalopathy CTOS, 12th Annual Meeting, Venice 2-4 November 2006
METHOTREXATE TOXICITY • Mucositis / Stomatitis • Bone marrow suppression • Nephrotoxicity • Hepatotoxicity • Dermatitis • Encephalopathy • Patient’s discomfort • Increased morbidity • Increased costs • Potentially reduced treatment efficacy CTOS, 12th Annual Meeting, Venice 2-4 November 2006
DELAYS IN CHEMOTHERAPY AND OUTCOME IN OSTEOSARCOMA CTOS, 12th Annual Meeting, Venice 2-4 November 2006
DELAYS IN CHEMOTHERAPY AND OUTCOME IN OSTEOSARCOMA • Frei at al. Am J Med, 1980 Chemotherapy response in osteosarcoma improves by increasing MTX dose and worsens by increasing the time between MTX administrations CTOS, 12th Annual Meeting, Venice 2-4 November 2006
DELAYS IN CHEMOTHERAPY AND OUTCOME IN OSTEOSARCOMA • Frei at al. Am J Med, 1980 Chemotherapy response in osteosarcoma improves by increasing MTX dose and worsens by increasing the time between MTX administrations • Delepine et al. Cancer, 1996 Dose intensity of MTX seems to be a major factor in predicting the outcome of patients with localised high grade osteosarcoma CTOS, 12th Annual Meeting, Venice 2-4 November 2006
DELAYS IN CHEMOTHERAPY AND OUTCOME IN OSTEOSARCOMA • Frei at al. Am J Med, 1980 Chemotherapy response in osteosarcoma improves by increasing MTX dose and worsens by increasing the time between MTX administrations • Delepine et al. Cancer, 1996 Dose intensity of MTX seems to be a major factor in predicting the outcome of patients with localised high grade osteosarcoma • French Tumour Study Group, Cancer, 1998 Delay in MTX course administration is a negative prognostic factor in osteosarcoma CTOS, 12th Annual Meeting, Venice 2-4 November 2006
DELAYS IN CHEMOTHERAPY AND OUTCOME IN OSTEOSARCOMA • Frei at al. Am J Med, 1980 Chemotherapy response in osteosarcoma improves by increasing MTX dose and worsens by increasing the time between MTX administrations • Delepine et al. Cancer, 1996 Dose intensity of MTX seems to be a major factor in predicting the outcome of patients with localised high grade osteosarcoma • French Tumour Study Group, Cancer, 1998 Delay in MTX course administration is a negative prognostic factor in osteosarcoma • Bacci et al. Oncol Rep, 2001 Avoiding reductions in MTX doses and /or delays in chemotherapy is crucial in osteosarcoma outcome CTOS, 12th Annual Meeting, Venice 2-4 November 2006
MAP (Methotrexate + Adriamycin+ cisPlatin) CTOS, 12th Annual Meeting, Venice 2-4 November 2006
OBJECTIVES AND METHODS • OBJECTIVE Incidence of delays in chemotherapy due to methotrexate toxicity in treatment of osteosarcoma CTOS, 12th Annual Meeting, Venice 2-4 November 2006
OBJECTIVES AND METHODS • OBJECTIVE Incidence of delays in chemotherapy due to methotrexate toxicity in treatment of osteosarcoma • METHODS - Patients treated with MAP between 2003 and January 2006 - Notes of 56 patients retrieved - Data collected on age, gender, chemotherapy dates, surgery dates, folinic acid rescue - Delayed courses identified, information collected on delays due to MTX toxicity - Applicable and non-applicable cycles CTOS, 12th Annual Meeting, Venice 2-4 November 2006
FOLINIC ACID RESCUE (FAR) REGIMENS • FAR regimen A - FAR starts at 24 hours and continues until MTX serum levels <0.2 µmol/L - FAR is adjusted according to MTX levels, 48 hours onwards CTOS, 12th Annual Meeting, Venice 2-4 November 2006
FOLINIC ACID RESCUE (FAR) REGIMENS • FAR regimen A - FAR starts at 24 hours and continues until MTX serum levels <0.2 µmol/L - FAR is adjusted according to MTX levels, 48 hours onwards • FAR regimen B - FAR starts at 24 hours and continues until MTX serum levels <0.2 µmol/L - FAR is adjusted according to MTX levels, 24 hoursonwards CTOS, 12th Annual Meeting, Venice 2-4 November 2006
FOLINIC ACID RESCUE (FAR) REGIMENS LATE • FAR regimen A - FAR starts at 24 hours and continues until MTX serum levels <0.2 µmol/L - FAR is adjusted according to MTX levels, 48 hours onwards • FAR regimen B - FAR starts at 24 hours and continues until MTX serum levels <0.2 µmol/L - FAR is adjusted according to MTX levels, 24 hoursonwards EARLY CTOS, 12th Annual Meeting, Venice 2-4 November 2006
METHODS CTOS, 12th Annual Meeting, Venice 2-4 November 2006
METHODS CTOS, 12th Annual Meeting, Venice 2-4 November 2006
METHODS CTOS, 12th Annual Meeting, Venice 2-4 November 2006
METHODS CTOS, 12th Annual Meeting, Venice 2-4 November 2006
METHODS CTOS, 12th Annual Meeting, Venice 2-4 November 2006
METHODS CTOS, 12th Annual Meeting, Venice 2-4 November 2006
RESULTS • Total number of patients: 56 • Median age: 20 years • M:F 1.6:1 • Total number of cycles received: 235 • Median number of cycles received per patient: 5 • Applicable cycles: 175 FAR regimen A: 98/175 (56%) FAR regimen B: 77/175 (44%) • Median number of applicable cycles received per patient: 4 • Median number of delayed cycles per patient: 1.5 • No deaths due to MTX toxicity CTOS, 12th Annual Meeting, Venice 2-4 November 2006
INCIDENCE OF DELAYED CHEMOTHERAPY CYCLES CTOS, 12th Annual Meeting, Venice 2-4 November 2006
INCIDENCE OF DELAYED CHEMOTHERAPY CYCLES CTOS, 12th Annual Meeting, Venice 2-4 November 2006
INCIDENCE OF DELAYED CHEMOTHERAPY CYCLES CTOS, 12th Annual Meeting, Venice 2-4 November 2006
INCIDENCE OF DELAYED CHEMOTHERAPY CYCLES CTOS, 12th Annual Meeting, Venice 2-4 November 2006
MTX-INDUCED DELAYS IN CHEMOTHERAPY CTOS, 12th Annual Meeting, Venice 2-4 November 2006
INCIDENCE OF DELAYS PER CYCLE CTOS, 12th Annual Meeting, Venice 2-4 November 2006
AGE AND DELAYED CYCLES CTOS, 12th Annual Meeting, Venice 2-4 November 2006
AGE AND DELAYED CYCLES CTOS, 12th Annual Meeting, Venice 2-4 November 2006
AGE AND DELAYED CYCLES CTOS, 12th Annual Meeting, Venice 2-4 November 2006
AGE AND DELAYED CYCLES CTOS, 12th Annual Meeting, Venice 2-4 November 2006
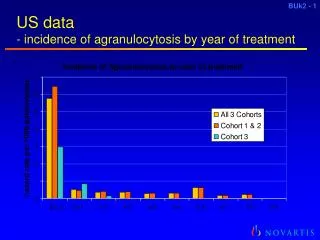
OMITTED MTX COURSES AND EARLY DISCONTINUATION OF MAP • OMITTED MTX COURSES - of 350 planned MTX courses, 5% (16/350) were omitted due to MTX toxicity • MAP EARLY DISCONTINUATION - in 10% (6/56) of the patients MAP treatment was discontinued early due to MTX toxicity CTOS, 12th Annual Meeting, Venice 2-4 November 2006
CONCLUSIONS • MTX-induced chemotherapy delays have decreased by ~20% with early FAR adjustment (57% vs 47%) • Median number of delayed chemotherapy cycles per patient: 1.5/4 • Incidence of MTX-induced chemotherapy delays is still high • Improving rescue from MTX-toxicity is a worthwhile goal CTOS, 12th Annual Meeting, Venice 2-4 November 2006
CONCLUSIONS • MTX-induced chemotherapy delays have decreased by ~20% with early FAR adjustment (57% vs 47%) • Median number of delayed chemotherapy cycles per patient: 1.5/4 • Incidence of MTX-induced chemotherapy delays is still high • Improving rescue from MTX-toxicity is a worthwhile goal CTOS, 12th Annual Meeting, Venice 2-4 November 2006