
Estimating Costs of Parkinson’s Disease in the United States
E N D
Presentation Transcript
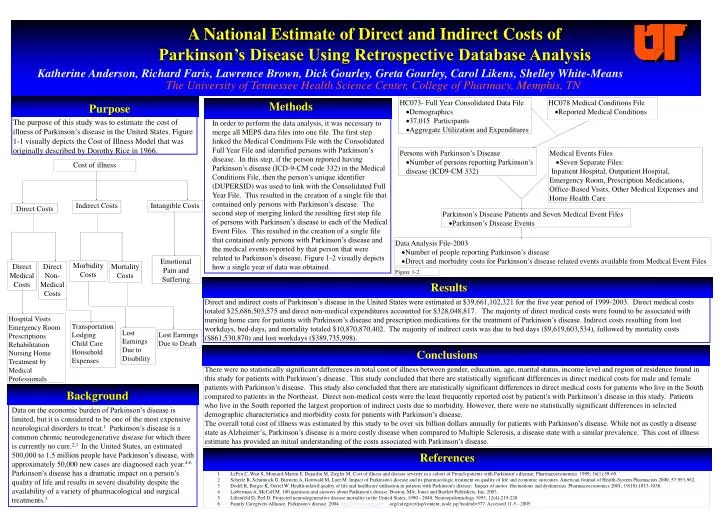
A National Estimate of Direct and Indirect Costs of Parkinson’s Disease Using Retrospective Database Analysis Katherine Anderson, Richard Faris, Lawrence Brown, Dick Gourley, Greta Gourley, Carol Likens, Shelley White-Means The University of Tennessee Health Science Center, College of Pharmacy, Memphis, TN • HC073- Full Year Consolidated Data File • Demographics • 37,015 Participants • Aggregate Utilization and Expenditures • HC078 Medical Conditions File • Reported Medical Conditions Methods Purpose The purpose of this study was to estimate the cost of illness of Parkinson’s disease in the United States. Figure 1-1 visually depicts the Cost of Illness Model that was originally described by Dorothy Rice in 1966. In order to perform the data analysis, it was necessary to merge all MEPS data files into one file. The first step linked the Medical Conditions File with the Consolidated Full Year File and identified persons with Parkinson’s disease. In this step, if the person reported having Parkinson’s disease (ICD-9-CM code 332) in the Medical Conditions File, then the person’s unique identifier (DUPERSID) was used to link with the Consolidated Full Year File. This resulted in the creation of a single file that contained only persons with Parkinson’s disease. The second step of merging linked the resulting first step file of persons with Parkinson’s disease to each of the Medical Event Files. This resulted in the creation of a single file that contained only persons with Parkinson’s disease and the medical events reported by that person that were related to Parkinson’s disease. Figure 1-2 visually depicts how a single year of data was obtained. • Persons with Parkinson’s Disease • Number of persons reporting Parkinson’s disease (ICD9-CM 332) • Medical Events Files • Seven Separate Files: • Inpatient Hospital, Outpatient Hospital, Emergency Room, Prescription Medications, Office-Based Visits, Other Medical Expenses and Home Health Care Cost of illness Indirect Costs Intangible Costs Direct Costs • Parkinson’s Disease Patients and Seven Medical Event Files • Parkinson’s Disease Events • Data Analysis File-2003 • Number of people reporting Parkinson’s disease • Direct and morbidity costs for Parkinson’s disease related events available from Medical Event Files Emotional Pain and Suffering Morbidity Costs Direct Medical Costs Direct Non-Medical Costs Mortality Costs Figure 1-2 Results Direct and indirect costs of Parkinson’s disease in the United States were estimated at $39,661,102,321 for the five year period of 1999-2003. Direct medical costs totaled $25,686,503,575 and direct non-medical expenditures accounted for $328,048,817. The majority of direct medical costs were found to be associated with nursing home care for patients with Parkinson’s disease and prescription medications for the treatment of Parkinson’s disease. Indirect costs resulting from lost workdays, bed-days, and mortality totaled $10,870,870,402. The majority of indirect costs was due to bed days ($9,619,603,534), followed by mortality costs ($861,530,870) and lost workdays ($389,735,998). Hospital Visits Emergency Room Prescriptions Rehabilitation Nursing Home Treatment by Medical Professionals Transportation Lodging Child Care Household Expenses Lost Earnings Due to Disability Lost Earnings Due to Death Conclusions There were no statistically significant differences in total cost of illness between gender, education, age, marital status, income level and region of residence found in this study for patients with Parkinson’s disease. This study concluded that there are statistically significant differences in direct medical costs for male and female patients with Parkinson’s disease. This study also concluded that there are statistically significant differences in direct medical costs for patients who live in the South compared to patients in the Northeast. Direct non-medical costs were the least frequently reported cost by patient’s with Parkinson’s disease in this study. Patients who live in the South reported the largest proportion of indirect costs due to morbidity. However, there were no statistically significant differences in selected demographic characteristics and morbidity costs for patients with Parkinson’s disease. The overall total cost of illness was estimated by this study to be over six billion dollars annually for patients with Parkinson’s disease. While not as costly a disease state as Alzheimer’s, Parkinson’s disease is a more costly disease when compared to Multiple Sclerosis, a disease state with a similar prevalence. This cost of illness estimate has provided an initial understanding of the costs associated with Parkinson’s disease. Background Data on the economic burden of Parkinson’s disease is limited, but it is considered to be one of the most expensive neurological disorders to treat.1 Parkinson’s disease is a common chronic neurodegenerative disease for which there is currently no cure.2,3 In the United States, an estimated 500,000 to 1.5 million people have Parkinson’s disease, with approximately 50,000 new cases are diagnosed each year.4-6 Parkinson’s disease has a dramatic impact on a person’s quality of life and results in severe disability despite the availability of a variety of pharmacological and surgical treatments.3 References 1 LePen C, Wait S, Moutard-Martin F, Dujardin M, Ziegler M. Cost of illness and disease severity in a cohort of French patients with Parkinson‘s disease. Pharmacoeconomics 1999; 16(1):59-69. 2 Scheife R, Schumock G, Burstein A, Gottwald M, Luer M. Impact of Parkinson's disease and its pharmacologic treatment on quality of life and economic outcomes. American Journal of Health-System Pharmacists 2000; 57:953-962. 3 Dodel R, Berger K, Oertel W. Health-related quality of life and healthcare utilisation in patients with Parkinson's disease: Impact of motor fluctuations and dyskinesias. Pharmacoeconomics 2001; 19(10):1013-1038. 4 Lieberman A, McCall M. 100 questions and answers about Parkinson's disease. Boston, MA: Jones and Bartlett Publishers, Inc, 2003. 5 Lilienfeld D, Perl D. Projected neurodegenerative disease mortality in the United States, 1990 - 2040. Neuroepidemiology 1993; 12(4):219-228. 6 Family Caregivers Alliance. Parkinson's disease. 2004. http://www.caregiver .org/caregiver/jsp/content_node.jsp?nodeid=577. Accessed 11-5 - 2005


















