BACTERIA
210 likes | 326 Views
Bacteria, although often harmless to humans, can lead to diseases through toxins they produce. These single-celled prokaryotes lack a nucleus and organelles, allowing for rapid reproduction and high mutation rates, which contribute to their evolution. Bacteria thrive in diverse environments and can exchange DNA, enhancing their adaptability. This high genetic diversity can result in rapid evolution due to the pressures of environmental changes and the competition. Understanding bacteria helps recognize their role in health and disease, including their capabilities of resistance and adaptation.

BACTERIA
E N D
Presentation Transcript
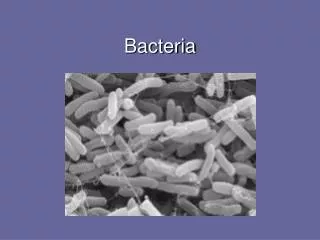
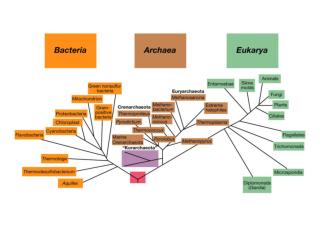
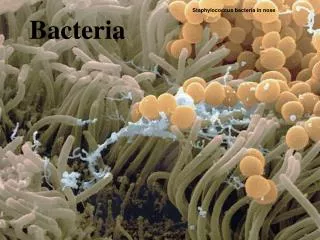
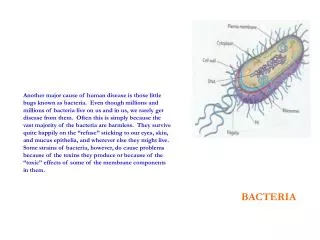
Another major cause of human disease is those little bugs known as bacteria. Even though millions and millions of bacteria live on us and in us, we rarely get disease from them. Often this is simply because the vast majority of the bacteria are harmless. They survive quite happily on the “refuse” sticking to our eyes, skin, and mucus epithelia, and wherever else they might live. Some strains of bacteria, however, do cause problems because of the toxins they produce or because of the “toxic” effects of some of the membrane components in them. BACTERIA
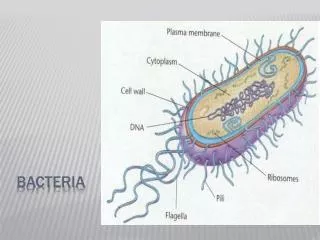
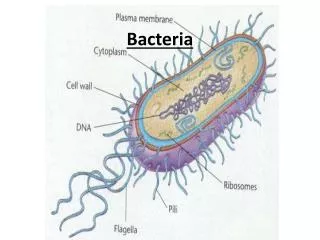
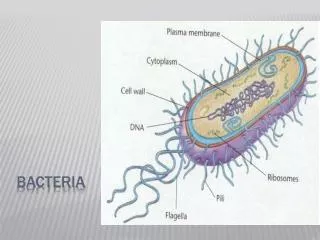
Procaryote - single cell - no nuclear envelope no discrete organelles - inclusions (contain CHO, Protein, Lipids) - cell wall multiple layers to protect cell membrane flagella (movement) pili (attatchment & exchange components - excrete protein toxins (exotoxins) - LPS (endotoxin)
Bacteria are prokaryotes, which means they have no nucleus nor any other observable organelles. All their metabolic enzymes and DNA kind of float about in their cytosol. The metabolic enzymes and DNA are mostly protected from environmental damage from such things as toxins and radiation by a cell wall made up of many complex proteins and lipids which closely surrounds the bacterial cell membrane. Because bacteria are single-celled animals, they simply excrete their waste into their environment. In some cases, their excretions aren’t waste, but toxic molecules meant to kill other small things in order to obtain a source of food. Of the trillions of bacteria that live on our skin and throughout our respiratory and GI tracts, they rarely grow to such massive populations that can cause harm because they kill and eat each other - thereby keeping “everyone in check”.
Bacteria (DNA, propagation - diversity) Bacteria divide by binary fission, meaning their DNA is duplicated “exactly” and the resulting 2 cells after division are “identical”... with a division cycle occurring anywhere from every 15 minutes to one every several hours Not only can bacteria duplicate their DNA for cell division to produce 2 daughter cells with the same DNA, they also can pick up plasmid DNA directly from other bacteria through their pili - effectively increasing the diversity of their DNA before dividing Bacteria also have an interesting habit of picking up snips of DNA from their environment and (like us) from viruses. This is another interesting concept because if any DNA pieces are picked up that actually code for a useful protein, the bacteria immediately gains that function... High-speed evolution, if you will! Bacterial DNA also has no introns; unlike human DNA. All the DNA bases code for something useful. This means that a mutation somewhere will affect a gene. Unlike human DNA which has many exons & introns and many regions of DNA that do not code for functional genes; therefor human DNA can afford to mutate many times because the odds are that most mutations happen in a non-coding part of the DNA strands.
Bacterial DNA and mutation Because bacteria have no nucleus, their DNA is in somewhat a more dangerous location than ours. Imagine some bacteria living on your skin while you are sitting in the sun. The UV radiation is causing the production of oxygen radicals in those cells that it can penetrate through. The bacteria wall will certainly absorb some of the radiation but any that gets through will have direct access to damage the DNA. Compare this to your own more fragile skin cells... The UV radiation must pass through several layers of dead cells on the surface of your skin and then through a layer of highly keratinized connective tissue (epidermis) before penetrating through several layers of the various cells that make up our dermis. Only after penetrating through these layers of cells can the UV radiation that makes it through actually penetrate into the committed stem cells in the lowest layer of our skin. And, even though some of the radiation actually makes it through to these cells, it still must penetrate through the various intervening membranes of the cell membrane, rER, sER, mitochondria, and nuclear membrane. There are a lot of targets for UV damage in human skin cells that get in the way long before the DNA of a dividing stem cell will actually get damaged compared to the number of targets between a bacterial cell wall and the DNA inside. This has serious implications for the production of mutations and the evolution of bacteria.
Bacteria (DNA, propagation & evolution) So when you put together high duplication rates and high mutation rates and high DNA transfer rates, you get the end result that bacteria in general can evolve very quickly... Population density of a typical colony is usually >> 109 With a mutation rate ~ 10-8 mutations / division AND: 1 x 108 bacteria to 2 x 108 bacteria in a (very small) colony this would result in ~1 mutant bacteria produced every time the colony divides once (doubles) with normally >> 109 bacteria / colony this would result in > 10 mutants / 15 minutes & doubling every 15 minutes... Means an awful lot of mutant bacteria being produced every single day. producing one mutant with a selective advantage (say drug resistance) is highly likely and because bacteria exchange DNA a high adaptation rate of resistance for all bacteria in colony is highly likely
Common Diseases Caused by Bacteria Food/Water Poisoning Vibrio cholera Staphylococcus aureus Escherichia coli Clostridium perfringes Salmonella typhi Shigella dysenteriae Skin Lesions (folliculitis, impetego, boils, pimples, carbuncles) Staphylococcus aureus Staphylococcus pyogenes Proprionibacterium acnes Strep Throat / Tonsillitis Streptococcus pyogenes Pneumonia Escherichia coli Staphylococcus aureus Staphylococcus pyogenes Streptococcus pyogenes Staphylococcus pneumonia
We get exposed to bacteria that float in the air every time we breathe and to bacteria in our drinking water every time we drink and to bacteria on our skin every time we touch something, and then touch our face. Water-borne bacteria typically live on the tiny bits of sewage, animal feces, and dead things that are in the water. In most Western countries, water and sewage treatment programs minimize the incidences of water poisoning. In countries where water-treatment is minimal or non-existent, water poisoning is common and a serious issue for small children. When these same bacteria live on food items that have been left out in the open, and we then eat them, we can suffer food poisoning. Symptoms of each are dependent on the specific type of bacteria and the effect of their toxins; reviewed later.
Lyme Disease Boreelia burgdorferi Rocky Mountain Spotted Fever Rickettsia ricketsia Anthrax Bacillus anthracis Meningitis Haemophilus influenza Staphylococcus pneumonia Neisseria meningitidis Streptococcus pyogenes Common STD’s Syphilis Treponema pallidum Gonorrhea Neisseria gonorrhoeae Chlamydia Chlamydia trachomatis
Some bacteria produce toxins which create pores in cell membranes, allowing electrolytes and other compounds to leak out (or in). This can seriously disrupt cell function. If the pores are large enough then the membrane will rupture and the cell will die. If you kill off enough cells this way you might go along with them. Another possibility is for bacteria to secrete digestive enzymes. These will digest membranes of nearby cells and kill them (sometimes extremely quickly). Some bacteria don’t secrete toxins but rather, simply stimulate an inflammatory response. Very often the response is stimulated by the lipopolysaccharide (LPS) in the bacteria’s outer cell membrane. The LPS directly stimulates macrophages to release cytokines (lots of them) and the inflammatory race then gets started. With a large overgrowth of high LPS bacteria in the intestine it is possible to get such massive inflammation within the abdominal cavity that blood volume drops, blood pressure drops, and you then die from it (think ruptured appendix or septicemia). One other not-very-cute way for bacteria to kill you is to provoke a massive systemic inflammatory response. Some bacteria proteins act as super-antigens. You already know that antigens stimulate T-cells and B-cells to proliferate and to release inflammatory cytokines. Normally just a tiny percentage of T-cells are affected by any antigen. Super-antigens, however, can stimulate as much as 20% of the entire population of T-cells. This can be disastrous when all of them release inflammatory cytokines at the same time. In essence, the massive systemic inflammatory response leads to total cardiovascular collapse (imagine what would happen when the blood-flow changes that typically happen locally, suddenly occur all over your entire body at the same time - think TSS). The following slides outline in point form a series of infectious bacteria and the mechanisms of their effects.
Escherichia coli - lives on skin, intestines - food poisoning, diarrhea, pneumonia LabileToxin (LT) – activated by host protease - Stimulates adenylate cyclase - Ribosylation of G-proteins - continual cAMP, cGMP production - Cl-, Na+, water loss StableToxin (ST) - Stimulates guanylate cyclase - cGMP production - Cl- loss No antibiotic treatment recommended due to exacerbation of symptoms.
Escherichia coli 0157:H7 - intestines - food poisoning, diarrhea, hemorrhagic colitis Verotoxin / shiga-like toxin - adhere to intestinal cells - penetrate cells and inhibit protein synthesis = no repair of damage No antibiotic treatment recommended due to exacerbation of symptoms.
Staphylococcus aureus - skin, nasal mucosa, mouth, throat, vagina - food poisoning, impetigo, boils, endocarditis, pneumonia, septic shock, toxic shock syndrome A toxin - membrane damage - fibrin clot - release of inflammatory cytokines Enterotoxins SE-A through SE-G, TSST-1 (Super Antigens) - stimulate t cells directly (~20% activation vs usual 0.01%) - severe diarrhea, vomiting (SE-series) - cardiovascular collapse - kidney (and other organs) failure Penicillin resistant – vancomycin & nefcillin effective
Streptococcus pyogenes - mouth, throat, urethra, vagina - strep throat, tonsilitis, meningitis, pneumonia, toxic shock like syndrome, necrotizing fasciitis Erythrogenic / pyogenic toxin (Super Antigens – TS like) - stimulate t cells directly (~20% activation vs usual 0.01%) - severe diarrhea, vomiting - cardiovascular collapse - kidney (and other organs) failure Cysteine Protease (necrotizing fasciitis) - degrades proteins with cysteine Invasins lyse RBC’s, phagocytes, & others Penicillin effective
Chlamydia trachomatis - mucosal epithelia of urogenital tract but can invade & incubate inside the cells and break out - Chlamidia - inflammation / discharge (mucus / pus) - Azithromycin, amoxicillin, doxycycline effective Neisseria gonorrhoeae - mucosal epithelia of urogenital tract - gonorrhea - toxin produces mitochondrial damage - induces apoptosis - Penicillin partially effective; Ceftriaxone, Spectinomycin effective Treponema pallidum - any tissue - route of transmission is sexual – 30% progress to syphilis (remainder latent) - No adaptive immunity - toxin inhibits DNA synthesis / protein synthesis - lipoprotein stimulates macrophages / inflammation - chancre - rash (flu w/ possible meningitis) - gumma (30%) - Penicillin effective
This last series of slides illustrates how a bacteria that releases no toxins can produce disease through an inflammatory response
Mycobacterium tuberculosis Initial exposure to Mycobacterium tuberculosis leads to phagocytosis by alveolar and interstitial macrophages with release of inflammatory molecules by the stimulated macrophages
M. tuberculosis do not secrete toxins, they do not have an LPS component to stimulate macrophages to a “high degree”, and they are very hard to digest; therefore they can live inside macrophages and stimulate a “weak” adaptive immune response ROS attack leads to calcium entry and activation of PLA2 and production of PG’s, TX’s, & LT’s. Activated macrophages migrate to lymph to interact with t-cells to produce cell-mediated immune response. In response to cytokines cellular adhesion molecules are synthesized to attract and activate circulating neutrophils and monocytes.
A full-blown inflammatory attack on M. tuberculosis is initiated with the recruitment of large numbers of neutrophils and macrophages. Collagen production by fibroblasts and fibrinogen production by epithelial cells is greatly stimulated and COX-2 enzymes are induced. Cellular damage by ROS leads to cellular necrosis, DNA damage, and activation of AP-1 while T cell activation of macrophages leads to their death by apoptosis (killing the bacteria as well).
A fibrotic granuloma is formed from the necrotic cells, apoptotic cells, and infected macrophages. The granuloma effectively walls off the infected macrophages (and dead/dying cells) from the healthy tissue and prevents further inflammatory responses. When the infected macrophages die, further inflammatory responses will be initiated by the released bacteria. Pulmonary function is progressively compromised with each subsequent infection and fibrotic response. Stem cells in the area proliferate in response to the cellular necrosis to replace the destroyed pulmonary cells. Isoniazid, rifampin, pyrazinamide, ethambutol are partially effective.
Prevention tactics - Stay clean; wash hands and face frequently - Wash any cut or abrasion thoroughly with soap/water & antiseptic and keep covered/clean - Avoid close contact with infected persons - If infected: use appropriate antibiotics (as indicated) & treat symptoms - Avoid all use of antibiotics unless absolutely necessary