Download
1 / 39
390 likes | 1.22k Views
Mechanical heart valves and Anticoagulation. Dr. Alkesh ZALA Basic Physician trainee, Dept. of Cardiology, John Hunter hospital. Today’s discussion:. Case review The currently Available and most commonly Used mechanical prostheses. What determines the Choice of valves?

E N D
Mechanical heart valves and Anticoagulation Dr. Alkesh ZALA Basic Physician trainee, Dept. of Cardiology, John Hunter hospital.
Today’s discussion: Case review The currently Available and most commonly Used mechanical prostheses. What determines the Choice of valves? Risk of Valve Thrombosis WITHOUT Anticoagulation What are the INR Targets for these valves? Are the New Generation Valves Really LESS THORMBOGENIC?
CASE 75 year old lady with subdural bleed On warfarin for st. Jude’s bileaflet AVR alond with Bentall procedure in 2003 2007 – Embolic vertebrobassilar embolic stroke – Valve blammed THOUGH INR 3.2 Aspirin added and INR target now 3.5 - 4 INR within target range on presentation Surgical drainage on presentation day 4 Heparin infusion on day 5 & Warfarin recommenced on regular dose on day 7 – TOO EARLY?
Day 9 – increasingly confused with headache. Repeat CT – Acute subdural with midline shift Urgent surgical drainage Repeat CT on day13 – subdural stable. No focal Neurological deficit Heparin started Cardiology involved with regards to anticoagulation advise Summary: Elderly lady with st. Jude’s bileaflet valve along with Bentall’s procedure. Prior probable embolic stroke related to the Mechanical valve Risk of valve thrombosis Vs Serious risk of intracranial bleeding
Weighing the risk of valve thormbosis and serious significant risk of recurrence of the intracranial bleed: - Go OFF anticoagulation for 1-2 weeks. - Warfarin restarted next week Uneventful recovery without any further complications. “Gamble - Turns Out To Be a Winner “ Or “A rational evidence based decision”
“An ideal Prosthetic valve” Unidirectional flow Durable : 40million cycles/year Blood compatible: no thrombus, embolus Central flow: Laminar not turbulent Closing not damaging blood cells Last but not the least important – It should be quiet
Evolution of Prosthetic Heart Valves The development of the original ball-and-cage valve design can be attributed to the bottle stopper in 1858 In the early 1950’s, it led to the idea of a prosthetic heart valve consisting of a cage with a mobile spherical poppet First implanted in a human in a closed procedure in September of 1952. In 1953, marked successful use of the heart and lung machine, paving the way for the 1st open heart operations
Early valves • In the 1960s, the Starr–Edwards ball-and-cage mechanical prosthesis became the standard replacement valve for nearly a decade. • The tilting disc valve became more widely used in the 1970s to overcome some of the inherent problems of the ball-and-cage model. • Both of these designs, however, were plagued by hemodynamic limitations and thromboembolic complications. • In the 1980s, the St. Jude Medical bileaflet prosthesis supplanted the earlier devices as the most commonly implanted prosthetic heart valve. Since then, additional bileaflet devices with numerous design modifications have been developed and continue to be used today.
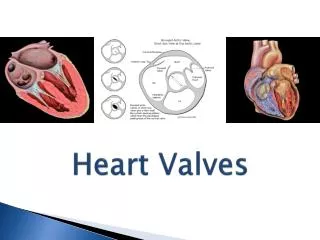
Different types of prosthetic valves. A, Bileaflet mechanical valve (St. Jude Medical). B, Monoleaflet mechanical valve (Medtronic-Hall). C, Caged ball valve (Starr-Edwards,). D, Stented porcine bioprosthesis (Medtronic Mosaic). E, Stented pericardial bioprosthesis (Carpentier-Edwards Magna). F, Stentless porcine bioprosthesis (Medtronic Freestyle). G, Transcatheter bioprosthesis expanded over a balloon (Edwards SAPIEN). H, Self-expandable percutaneous bioprosthesis (CoreValve,)edtronic).
Bileaflet valves Two semicircular leaflets that rotate about struts attached to the valve housing Good hemodynamic performance - improved flow characteristics, lower transvalvular pressure gradients, less blood flow turbulence, improved hemodynamics at a given annular diameter, a larger orifice area and low bulk and flat profile the least thrombogenic of the artificial valves most commonly implanted mechanical valves
However, inspite of improved design and haemodynamics – still haunted by numerous complications and the most dreaded one of valve thrombosis
Why not always use a Bioprosthetic valve !! Developed primarily to overcome the risk of thromboembolism that is inherent in all mechanical prosthetic valves Major problem – DURABILITY. Cuspal tears, degeneration, fibrin deposition, perforation, fibrosis, and calcification. Rate of tissue failure – by 10 years 30% and upto 60% by 15 years.
Choice of Valves Major task is to weigh the advantage of durability and the disadvantages of the risks of thromboembolism and anticoagulant treatment inherent with mechanical valves The next step is to choose a prosthesis model that provides superior hemodynamic performance to prevent prosthesis-patient mismatch (PPM) and thereby minimize postoperative trans-prosthetic gradients.
Criteria for selection of an aortic valve in patients undergoing aortic valve replacement (AVR)ACC/AHA guideline Data from Bonow, RO, Carabello, BA, Chatterjee, K, et al. ACC/AHA 2006 guidelines for the management of patients with valvular heart disease. A report of the Force on Practice Guidelines (Writing committee to revise the 1998 guidelines for thAmerican College of Cardiology/American Heart Association Task e management of patients with valvular heart disease). J Am Coll Cardiol 2006; 48:e1.
Criteria for selection of an Mitral valve in patients undergoing Mitral valve replacement (MVR)ACC/AHA guideline Data from Bonow, RO, Carabello, BA, Chatterjee, K, et al. ACC/AHA 2006 guidelines for the management of patients with valvular heart disease. A report of the Force on Practice Guidelines (Writing committee to revise the 1998 guidelines for thAmerican College of Cardiology/American Heart Association Task e management of patients with valvular heart disease). J Am Coll Cardiol 2006; 48:e1.
JHH Choice Courtesy: Dr. Taranpreet Singh Cardiothoracic surgeon, John Hunter Hospital • Mechanical valves represent about 5 – 10% of total valve replacement? Reason • Preferred mechanical valve – Bileaflet valve • Mechanical valves – Mitral > Aortic (However, Repair preferred over Replacement) • Apart from co-morbidities and Patient preference • AVR- Age 60 • MVR – Age 70
Thrombosis with Mechanical valve • Mechanical prostheses remains burdened with the risk of thrombosis – potentially fatal • Valve thrombosis is any thrombus in the absence of infection attached to or near an operated valve that occludes part of the blood flow path or that interferes with the function of the valve. • Risk factors: • inadequate or discontinued anticoagulant therapy • previous endocarditis • the prosthetic valve model used • LV dysfunction, LA dilatation • Hypercoagulable states
Prosthesis Thrombogenicity Low: St Jude Medical, On-X, Carbomedics, Medtronic Hall; Medium: bileaflet valves with insufficient data, Bjork-Shiley; High: Lillehei-Kaster, Omniscience, Starr-Edwards. Philippe Pibarot, P. et al, Selection of the Optimal Prosthesis and Long-Term Management. Circulation. 2009; 119: 1034-1048
Rate of thrombosis In absence of anticoagulation: 8.6 per 100 patient-years. With anticoagulation: risk is reduced to 1% to 3% per year. Valve thrombosis is increased with valves in the mitral position. Highest in the Tricuspid position. ?? Rate with remote valves Ref: Hurst's the Heart, 12th Edition
ACC/AHA guideline summary: Treatment of prosthetic heart valve thrombosis Bonow, RO, Carabello, BA, Chatterjee, K, et al. ACC/AHA 2006 guidelines for the management of patients with valvular heart disease. A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing committee to revise the 1998 guidelines for the management of patients with valvular heart disease). J Am Coll Cardiol 2006; 48:e1.
Anticoagulation guidelines ACC/AHA guideline summary: Antithrombotic therapy in patients with mechanical heart valves Bonow RO, Carabello BA, Chatterjee K, et al. 2008 Focused update incorporated into the ACC/AHA 2006 guidelines for the management of patients with valvular heart disease. A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing committee to revise the 1998 guidelines for the management of patients with valvular heart disease). Circulation 2008; 118:e523.
European College of Cardiology guideline Butchart, EG, Gohlke-Barwolf, C, Antunes, MJ, et al. Recommendations for the management of patients after heart valve surgery. Eur Heart J 2005; 26:2463.
The AREVA trial compared moderate anticoagulation (INR 2.0–3.0) to the usual regimen of INR 3.0–4.5. A similar risk in thromboembolic events was found in both arms, whereas the bleeding risk was higher in the high intensity group Acar J, Iung B, Boissel JP et al. AREVA. Multicenter randomized trial comparison of low-dose versus standard-dose anticoagulation in patients with mechanical prosthetic heart valves . Circulation 1996; 94: 2107 12.
International Normalized Ratio (INR)–specific incidence of all adverse events in patients with mechanical valves (all episodes of thromboembolism, all major bleeding episodes, and unclassified stroke) according to INR (A). The dotted lines represent the 95% confidence interval and according to INR, age, and position of valve (B). Incidence of thromboembolic events according to INR and patient age (upper graph) or prosthesis position (lower graph). S.C. Cannegieter, F.R. Rosendaal, A.R. Wintzen, F.J.M. van der Meer, J.P. Vandenbroucke, and E. Briet N Engl J Med 1995; 333:11-17July 6, 1995
LOWERING-IT trial established that the proposed LOW-INR target is safe and feasible in low-risk patients after bileaflet aortic mechanical valve replacement. prospective open-label, single-center, randomized controlled trial: age 20 to 60 years, a single-valve replacement with a bileaflet valve in the aortic position Low risk 396 patients: 197 in low INR (1.5-2.5) AND 199 in standard INR group (2.0 – 3.0). Results - similar thrombotic events and a significant reduction of bleeding occurrence in the low INR group Torella, M. Torella, D. LOWERing the INtensity of oral anticoaGulant Therapy in patients with bileaflet mechanical aortic valve replacement: Results from the “LOWERING-IT” Trial. American heart Journal – Volume 160, Issue 1 (July 2010)
Are new generation valves really less thrombogenic? All Mechanical valves models are vulnerable to thrombus formation due to high shear stress, stagnation, and flow separation. The quest to find a less thormbogenic valve was one of the prime driving force in the development of the newer heart valves Less thrombogenic materials and an improved valve and hinge design has reduced the propensity for thrombus formation and the need for aggressive anticoagulation.
A meta-analysis of 46 trial - a higher risk of embolic complications in patients with a caged-ball valve. The incidence of total thromboembolism was 30% lower for patients with a tilting disk valve, and 50% lower for patients with a bileaflet valve. Cannegieter SC, Rosendaal FR, Torn M. Oral anticoagulant treatment in patients with mechanical heart valves: how to reduce the risk of thromboembolic and bleeding complications. Journal of Internal Medicine,Volume 245, Issue 4, pages 369–374, April 1999
In the cohort study of 1608 patients with mechanical heart valves: a clearly higher risk of thromboembolism in patients with caged-ball valves. An incidence of 0.5 per 100 patient-years was found for the bileaflet valves, of 0.7 per 100 patient-years for the tilting disk valves, and of 2.5 per 100 patient-years for the caged-ball valves Cannegieter SC, Rosendaal FR, Wintzen AR, Van Der Meer Fjm, Vandenbroucke JP, Briët E. Optimal oral anticoagulant therapy in patients with mechanical heart valves. N Engl J Med 1995; 333: 11 17.
Guideline Which valves are less thormobogenic and safe to be managed with lower INR targets??
The quest continues… “Eight Commandments”: • Embolism Prevention • Durability • Ease and Security of Attachment • Preservation of Surrounding Tissue Function • Reduction of Turbulance • Reduction of Blood Trauma • Reduction of Noise • Use of Materials Compatible with Blood
References Acar J, Iung B, Boissel JP et al. AREVA. Multicenter randomized trial comparison of low-dose versus standard-dose anticoagulation in patients with mechanical prosthetic heart valves . Circulation 1996; 94: 2107 12. Bonow, RO, Carabello, BA, Chatterjee, K, et al. ACC/AHA 2006 guidelines for the management of patients with valvular heart disease. A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing committee to revise the 1998 guidelines for the management of patients with valvular heart disease). J Am CollCardiol 2006; 48:e1. Braunwald's Heart Disease - A Textbook of Cardiovascular Medicine, 9th ed. Cannegieter SC, Rosendaal FR, Wintzen AR, Van Der Meer Fjm, Vandenbroucke JP, Briët E. Optimal oral anticoagulant therapy in patients with mechanical heart valves. N Engl J Med 1995; 333: 11 17. Hurst's the Heart, 12th Edition Torella, M. Torella, D. LOWERing the INtensity of oral anticoaGulant Therapy in patients with bileaflet mechanical aortic valve replacement: Results from the “LOWERING-IT” Trial. American heart Journal – Volume 160, Issue 1 (July 2010) Uptodate