
Cohort Study Design in Epidemiology: Understanding Methods and Analysis
E N D
Presentation Transcript
COHORT STUDY Dr Santosh K Yatnatti
EPIDEMIOLOGY: Study Designs • Ecological Studies • Cross sectional (Prevalence) studies • Case-Control Studies • Cohort Studies (Prospective, Longitudinal, Incidence) • Intervention Studies (experiments)
Hypothesis Medical school performance has no effect on the future career of a doctor
Introduction • What is a cohort • Analytical study • Starts with people free of disease • Assesses exposure at “baseline” • Cohort is followed up • Proceeds from cause to effect • Assesses disease status at “follow-up” • two measurement (baseline and follow-up) • individual is the unit of observation and analysis
DESIGN OF A COHORT STUDY TIME direction of enquiry disease exposed Population People without the disease no disease Some sort of sample disease Not exposed no disease
Cohort study Framework Disease Y N a b a+b Y Exposed cohort Exposure c d c+d N Non-exposed cohort a+c b+d N
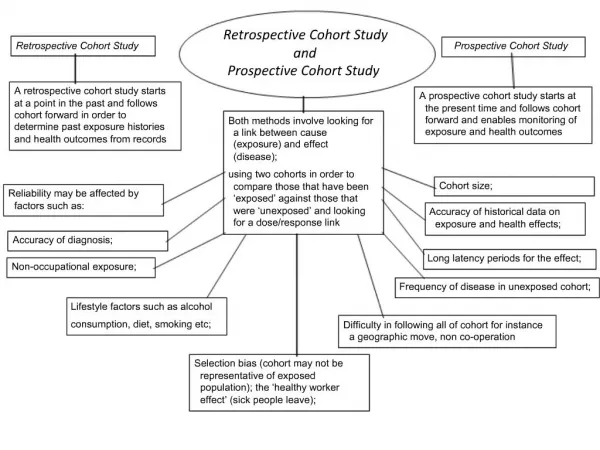
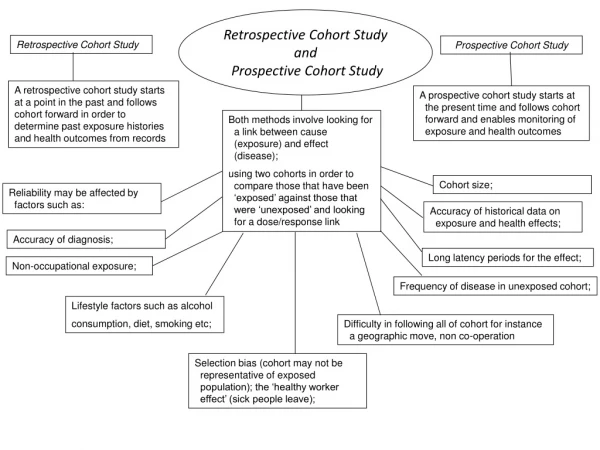
Type of Cohort studies • Prospective: start with exposed and unexposed groups, wait for the outcome
Type of Cohort studies • Retrospective: both exposure and outcome have already happened, but groups are still made based on exposed or unexposed Past Present Disease + Disease - Risk + Disease + Disease - Risk -
Criteria of a cohort • Free of disease even subclinical • Both groups equally susceptible • Both groups comparable • Diagnostic and eligibility criteria defined beforehand
Cohort studies • Studies whether exposure to a “risk factor” is associated with a subsequent “outcome” • Select two populations who seem the same except for the hypothesized risk factor • Follow them and see how many have the outcome or disease • Important concept: Start with the risk, then look for the outcome
Elements of cohort study A. Selection of study subjects • The general population (or a sample of it) • Framingham heart study • A group that is easy to follow-up • Doll and Hill study • With some special exposure (especially rare exposures) • Occupational exposures
Elements of cohort study B. Obtaining data on exposure • Interviews or mailed questionnaires • Records • Medical examination • Environmental surveys • Data collected should classify the cohort on presence or absence and degree of exposure
Elements of cohort study C. Selection of comparison groups • Internal comparison • Stratify by level of exposure • Separate cohort • As similar as possible to exposed cohort • education, income, gender, race, geographic location • Comparison with available population rates
Elements of cohort study D. Follow up • Periodic medical examination • Reviewing records • Death records • Home visits, questionnaires, telephone calls
Elements of cohort study E. Analysis Disease Y N a b a+b Y Exposed cohort Exposure c d c+d N Non-exposed cohort a+c b+d N • Incidence among exposed • Incidence among non-exposed • Relative risk • Attributable rsk
INCIDENCE OF DIESEASE (DEATH ) AMONG EXPOSDED RELATIVE RISK = INCIDENCE OF DISEASE (DEATH) AMONG NON - EXPOSED RR OF LUNG CANCER = 10 / 1 = 10 SMOKERS ARE 10 TIMES AT GREATER RISK OF DEVELOPING LUNG CANCER THAN NON SMOKERS
ATTRIBUTABLE RISK: • EXPRESSED AS PERCENT INCIDENCE OF DISEASE RATE AMONG EXPOSED MINUS- INCIDENCE OF DISEASE RATE AMONG NON - EXPOSED x 100 INCIDENCE RATE AMONG EXPOSED = 10- 1 x 100 = 90% 10 TO WHAT EXTENT THE DISEASE UNDER STUDY CAN BE ATTRIBUTED TO EXPOSURE
determination of incidence and risk multiple exposures and multiple outcomes can establish cause - effect good when exposure is rare temporal relationship clear minimizes selection and information bias validity affected by losses to follow-up often requires large sample ineffective for rare diseases long time to complete expensive subject attrition confounding by other factors possible Cohort studies Strength Weakness
Potential biases in cohort studies • Selection (confounding) bias: have to match similar groups • Detection bias: measurement of outcomes needs to be objective and similar for both groups • Length-time bias: study has to be long enough for outcome to happen • Excursion bias: subjects may disappear or drop-out (lost to follow-up)
To Summarize Define the Cohort Selection of study population Get baseline exposure measurements Follow cohort for disease / outcome Additional exposures measured over time Analyse disease risk according to exposure