Cohort Study Designs
Cohort Study Designs. Ahmed Mandil Dept of Family & Community Medicine College of Medicine King Saud University. Headlines. Definitions Observational studies Characteristics Advantages, disadvantages, problems Examples Analysis. Observation Methods.

Cohort Study Designs
E N D
Presentation Transcript
Cohort Study Designs Ahmed Mandil Dept of Family & Community Medicine College of Medicine King Saud University
Headlines • Definitions • Observational studies • Characteristics • Advantages, disadvantages, problems • Examples • Analysis Cohort Studies
Observation Methods • Selected Units: individuals, groups • Study Populations: cross-sectional, longitudinal • Data collection timing: prospectively, retrospectively, combination • Data collection types: primary, secondary Cohort Studies
Study populations • Cross-sectional: where only ONE set of observations is collected for every unit in the study, at a certain point in time, disregarding the length of time of the study as a whole • Longitudinal: where TWO or MORE sets of observations are collected for every unit in the study, i.e. follow-up is involved in order to allow monitoring of a certain population (cohort) over a specified period of time. Such populations are AT RISK (disease-free) at the start of the study. Cohort Studies
Epidemiological Measures • Frequency measures: incidence; prevalence • Effect measures: risk ratio (relative risk); odds ratio • Impact measures: attributable fraction; prevented fraction Cohort Studies
Observational Designs • Exploratory: used when the state of knowledge about the phenomenon is poor: small scale; of limited duration. • Descriptive: used to formulate a certain hypothesis: small / large scale. Examples: case-studies; cross-sectional studies • Analytical: used to test hypotheses: small / large scale. Examples: case-control, cross-sectional, cohort. Cohort Studies
Cross-sectional Studies (I) (a) Characteristics: • A study to detect point prevalence • A reference population from which a random sample of chosen • Allows for stratification • Suitable for relatively frequent conditions • We are looking for both the disease and exposure status simultaneously Cohort Studies
Cross-sectional Studies (II) (b)Advantages: • Feasible, relatively easy to administer • Less time-consuming (compared to prospective cohort studies) • Less costly • Allows for studying several conditions /exposures at the same time • Useful for health planning Cohort Studies
Cross-sectional Studies (III) (c) Disadvantages: • Does not establish the temporal sequence of events necessary to suggest causal inference (temporal ambiguity) • Cannot distinguish risk from prognostic factors • Insufficient for studying of rare diseases (e.g. cancers) Cohort Studies
Case-control studies (I) (a) Characteristics: • Two distinct source populations • We know the disease status, looking for the exposure status • Ratio of case:controls chosen by the investigator, minimum is 1:1. • Usually cannot calculate frequency measures • We have to assume that the non-cases (control) group is representative of the same source population of cases, in order to make any causal inferences. Cohort Studies
Case-control studies (II) (b) Advantages: • Least expensive (smaller number of subjects involved) • Least time-consuming (relatively quick results) • Suitable for study of rare diseases Cohort Studies
Case-control studies (III) (c) Disadvantages: • Not suitable for rare exposures • Cannot calculate frequency measures • Liable to selection bias (controls are usually selected after occurrence of cases) • Liable to recall bias -> measurement error, especially with effect estimation. Cohort Studies
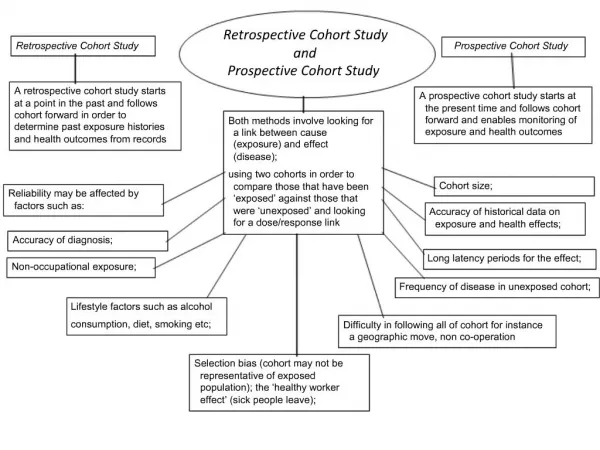
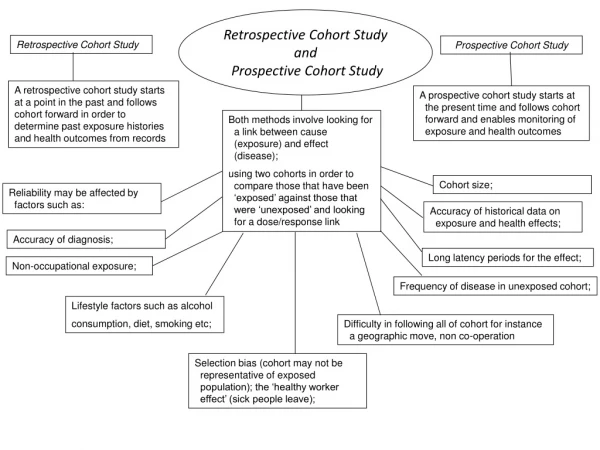
Cohort Studies (I) (a) Characteristics: • A “cohort” is a group of people, referred to as “disease-free population” or “population at risk” • A survey is first carried out to exclude prevalent cases from the cohort • A period of "follow-up“ is specified, for possible new cases' occurrence • We know the exposure status, looking for the disease status • Historical designs are preferred under occupational settings, for less frequent effects / exposures. Cohort Studies
Cohort Studies (II) Two types are recognized: • Prospective(longitudinal): forward in time follow-up study • Retrospective(historical): backward in time study (depends on records: medical / employment). This is the type preferred under occupational settings Cohort Studies
Cohort Studies (III) (b) Advantages: • No / little temporal ambiguity (suggests cause-effect relationship) • Calculation of incidence rates • Suitable for rare exposures • Factors associated with selection cannot influence disease status and hence the results. • Several outcomes can be studied, after follow-up starts. Cohort Studies
Cohort Studies (IV) ( c ) Disadvantages (of prospective): • Expensive • Time-consuming • May be impractical • Loss to follow-up may affect sample-size Cohort Studies
IDEAL COHORT An ideal cohort should be: • STABLE • COOPERATIVE • COMMITTED • WELL-INFORMED Cohort Studies
Examples of Study Cohorts • General population • Selected occupational groups, e.g. health professionals (physicians, nurses, lab technologists, etc), manufacturers of mercury batteries for vehicles; asbestos workers, miners, etc Cohort Studies
Sources of Cohorts • Population groups • Occupational settings (employment, medical records) • Hospital registers (medical records) • Death certificates Cohort Studies
Follow-up Techniques • PERIODICAL MEDICAL EXAMINATIONS AND MAILED QUESTIONNAIRES • DIRECT PERSONAL INTERVIEWS OR EXAMINATIONS • VIDEOCONFERENCE, NEIGHBORS, FRIENDS AND RELATIVES • LOST PERSONS CAN BE TRACED THROUGH THE LETTERS, FROM THEIR RELATIVES AND FRIENDS • MIGRATED COHORT SUBJECTS CAN ALSO BE TRACED THROUGH TRAVEL AND IMMIGRATION AUTHORITIES • DEAD PERSONS - LOCAL OR REGIONAL MORTALITY REGISTERS • OR DEATH CERTIFICATES Cohort Studies
Problems during Follow-up • FOLLOW-UP OF A LARGE GROUP • LIMITED RESOURCES • TIME SCARCITY • PAUCITY OF TRAINED PERSONNEL • ATTRITION, LOSS ON FOLLOW UP • ETHICAL CONCERNS Cohort Studies
Attrition Reduction • OBTAINING THE INFORMED CONSENT • RECORDING COMMITMENT TO CONTINUE AND COOPERATE IN THE STUDY • TRACING LOST SUBJECTS, TRYING TO INCLUDE THEM IN THE STUDY • CONSIDERING INFORMATION OF LOST PERSONS AT THE TIME OF ANALYSIS • KEEPING NON-RESPONSE AT A LOW LEVEL TO IMPROVE THE VALIDITY Cohort Studies
Examples of Cohort Studies • POPULATION-BASED • CARDIOVASCULAR • CHILD HEALTH • SPECIAL EXPOSURES • NON-POPULATION BASED • OCCUPATIONAL – for convenience • OCCUPATIONAL – to study the occupation • HEALTH CARE SETTINGS • VETERANS Cohort Studies
CARDIOVASCULAR DISEASE • USA: Framingham, MA; Tecumseh, MI; Evans county, GA; Muscatine, IA; Bogalusa, LA (children) • WHO MONICA (multi-center) • North Karelia, Norway Cohort Studies
Framingham Study (1951 – present time) • 1ST Step: Selection of cohorts • Initially, 5209 subjects were enrolled into the study • Currently, thousands of people are followed up, both for cardiovascular risk factors (e.g. high serum cholesterol, smoking, hypertension, BMI, etc) and possible outcomes Cohort Studies
CHILD HEALTH • National Birthday Trust Studies One week of births in England and Wales in 1946, 1958, 1970, etc • Project on Premature Infants All births < 1,500 g or < 32 weeks in a specific nation • The National Children Studyhttp://www.nichd.nih.gov/about/despr/despr.htm Cohort Studies
SPECIAL EXPOSURES • Atomic Bomb Casualty Commission (ABCC): Hiroshima and Nagasaki survivors (effects of radiation) • Dutch famine survivors (effects of starvation) • Seveso (effects of dioxin exposure) Cohort Studies
OCCUPATION-BASED COHORTS,CONVENIENT FOLLOW-UP • British Doctors Study (Doll – smoking) • Nurses Study (Speizer, Willett – many issues) • London civil servants (Marmot - SES) • Taiwanese civil servants (Beasley – liver cancer) Cohort Studies
OCCUPATION BASED, TO STUDY EXPOSURES • Benzene-workers (leukemia) • Coke-oven workers (lung cancer) • Asbestos workers (lung cancer) • Radium dial painters (oral cancer) Cohort Studies
SAMPLING FROM HEALTH CARE SETTINGS • National Collaborative Perinatal Project: Almost all pregnancies at 12 medical centers 1959-1966 – N about 50,000. (causes of CP) • Child Health and Development Studies: Kaiser-Permanente births (many issues) • Patients treated with radiation for polycythemia or ankylosing spondylitis (radiation and cancer) Cohort Studies
VETERANS • Mustard-gas poisoning from WW I (lung disease) • Vietnam Veterans (post-traumatic stress disorder, agent orange effects) • Gulf War Veterans (Gulf war syndrome) Cohort Studies
2x2 Table Cohort Studies
INCIDENCE RATES • INCIDENCE AMONG THE EXPOSED (NEW CASES AMONG THE SMOKERS) = (A/ A+B) • INCIDENCE AMONG THE NON-EXPOSED (NEW CASES AMONG THE NON-SMOKERS) = (C/ C+D ) Cohort Studies
Risk Calculations • Relative Risk or Risk Ratio (RR) (RR) = [A / (A+B)] / [C / C +D)] (incidence in the exposed (smokers) / incidence in the non-exposed (non-smokers) • Attributable risk (AR = excess risk/ incidence among the exposed (AETIOLOGICAL FRACTION) • Population attributable risk (PAR) = incidence in the total population minus incidence among the non-exposed. Cohort Studies
RR Interpretations • Unity: exposure has no effect on outcome in the studied population (cohort) • More than 1: exposed have a higher risk of developing the outcome, compared to the unexposed • Less than 1: either no relationship, or a “protective” one exists (e.g. effect of interventions, immunization, health education, management, etc) Cohort Studies
Frequency & Effect Measures Cohort Studies
Choice of study design • Status of existent knowledge • Occurrence of disease • Duration of latent period • Nature and availability of information • Available resources • Time constraints Cohort Studies
References • Last JM. A dictionary of epidemiology. 5th edition. New York, Oxford, Toronto: Oxford University Press, 2008. • Gordis L. Epidemiology. Third edition. Philadelphia, London, New York, Sydney: W.B. Saunders, 2004. • Beaglehole R, Bonita R, Kjellstrom T. 2nd edition. Basic epidemiology. Geneva: WHO, 2006. • Friis RH, Sellers TA. Epidemiology for public health practice. Gaithersburg, MD: Aspen Publishers, 1999. • Kelsey JL, Thompson WD, Evans AL. Methods in observational epidemiology. New York: Oxford University Press, 1986. Cohort Studies
Thank you for your kind attention Cohort Studies