Download

1 / 49
690 likes | 2.14k Views
Atrial Septal Defects. Imaging Conference December 10, 2008 Angela Morello, M.D. Clinical Importance:. Account for 10-15% of all congenital anomalies Most common congenital defect to present in adulthood. Embryology. Braunwald, 6th Edition. Types of ASD’s. Ostium Secundum Ostium Primum

E N D
Atrial Septal Defects Imaging Conference December 10, 2008 Angela Morello, M.D.
Clinical Importance: • Account for 10-15% of all congenital anomalies • Most common congenital defect to present in adulthood
Embryology Braunwald, 6th Edition
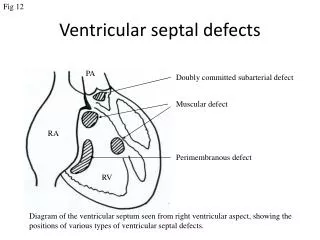
Types of ASD’s • Ostium Secundum • Ostium Primum • Sinus Venosus • Coronary sinus defects
Ostium Secundum ASD: • Most common type (70-75%) • 7% of all congenital heart defects = 5-6 cases per 10,000 live births • Female predominance 2:1 • Two common mechanisms: • Inadequate formation of septum secundum to not completely cover ostium secundum • Excessively large ostium secundum due to increased resorption; septum secundum can therefore not cover
Associated findings: • MVP (10-20%) • EKG abnormalities: • RAE • Prolonged PR interval • RAD (+100°) • rSR1 V1
Ostium Primum ASD: • Mostly in trisomy 21--> 1/800 live births • 40-50% Down’s pts have CHD: 65% of these are AV canal defects • Simplest form of AV canal defect (often associated with more advanced/complicated forms) • Female: male predominance is 1:1 • Located at most anterior and inferior aspect of the atrial septum • Formed by: • Ostium primum remains from septum primum • Usually sealed by fusion with endocardial cushions • Failure to fuse endocardial cushions--> associated AV valve abnormalities
Associated Findings: • Cleft anterior leaflet of mitral valve: MR • EKG findings: • PR prolongation • RAE • LAD • rSR1 in V1-V2
Sinus Venosus Defect: • Not truly considered an ASD • Only accounts for 10% of all “ASD’s”; 1% of all congenital defects in U.S. • Abnormal resorption of sinus venosus in development • Two types: • “Usual” type: upper atrial septum contingous with SVC • Less common: at junction of RA and IVC • Associated findings: • anomalous pulm venous drainage into RA or vena cavae • junctional/low atrial rhythm
Associated Findings: • Anomalous pulmonary venous drainage into RA or vena cavae • In “usual” type, RUPV drains to SVC • In less common type, RLPV drains to IVC • Junctional/low atrial rhythm
Pathophysiology: • Left to right shunting: Qp/Qs > 1.5/1.0 • Dependent on defect size and relative diastolic filling properties of the ventricles • Decreased ventricular compliance +/- increased left atrial pressure --> increase in shunting • Decrease ventricular compliance: • Systemic hypertension • Cardiomyopathy • MI • Increase LA pressure: • Mitral valve disease
Pathophysiology continued: • Flow in systole and diastole • Bulk of flow in diastole • Size of ASD determines volume of shunting
Presentation: • Often asymptomatic until 3-4th decade for moderate-large ASD • Fatigue • DOE: • 30% by 3rd decade • 75% by 5th decade • Atrial arrhythmias/SVT and R sided HF: • 10% by 4th decade • Increase therafter with age • Paradoxical Embolus: • Transient flow reversal (Valsalva/strain) • Pulmonary Hypertension
Physical Findings: • “Left atrialization” of JVP (A=V wave) • Hyperdynamic RV impulse • PA tap • S2 wide/fixed split • Grade II SEM: increased flow through TV
Echocardiographic Evaluation: • Subcostal view most reliable: US beam perpendicular to plane of IAS • Other views may have loss of signal from the atrial septum from parallel alignment • Secundum ASD: central portion of atrial septum (89% sensitivity) • Primum ASD: adjacent to AV valve annuli (100% sensitivity) • Sinus Venosus defects: difficult to visualize on TTE (44% sensitivity)
Echo in Secundum ASD: • Identify the following: • normal coronary sinus • entrance of pulmonary veins • intact primum portion of atrial septum • RV and RA size and function
Echo in Primum ASD: • “Drop-out” of inferior portion of IAS can be seen on apical 4 or subcostal views • TV NOT more apically positioned than MV; at same horizontal level • Color to differentiate from dilated coronary sinus • PW and CW Doppler to estimate RVSP and PA pressures
Associated findings by TTE: • Significant L--> R shunt • Right atrial enlargement • Right ventricular enlargement • Paradoxical septal motion (R sided volume overload)
Doppler Echocardiography: • Color Doppler can identify left to right flow • Subcostal view is best • Multiple views needed: • Low-velocity flow signal between atria • SVC flow along IAS can be mistaken for shunting • TR jet directed toward IAS
Doppler Echocardiography: • Volume Flow and Shunt calculation: • SV = CSA x VTI x 100 • SI = SV/BSA • CO = SV x HR/ 1000 • CI = CO/BSA
Doppler Echocardiography: • Shunt calculation: • Can be performed utilizing these equations to relate pulmonic CO and systemic CO • Qp = TVI pulm X PULd • Qs = TVI ot X LVOTd • Qp/Qs = shunt fraction • Significant usually if > 1.5/1.0 in ASD
Color Doppler: • Location and timing of flow critical • Flow from L--> R atrium in both systole and diastole • More prominent diastolic component • Can extend across open TV in diastole into RV • Flow acceleration on side of LA • Absolute velocity of flow less important
Contrast Echocardiography: • Microbubbles seen across IAS • Even if shunting predominantly L to R • RA pressure transiently > LA pressure • “Negative” contrast jet: • Flow from LA to RA appears as area with no echo contrast • Rarely needed for ASD - more useful for smaller shunts (PFO’s)
Indications for Intervention: • Asymptomatic in the presence of: • Right-sided cardiac dilatation • ASD > 5mm with no signs of spontaneous closure • Hemodynamics reserved for “borderline” cases • HD insignificant (Qp/Qs <1.5) - no closure required until later in life for embolism prevention after CVA • HD significant (Qp/Qs >1.5) - should be closed
Indications for Interventions continued… • In presence of PA HTN: • Defined as PAP > 2/3 systemic or PVR > 2/3 SVR • Closure can be recommended IF: • Net L--> R shunt of 1.5:1 or greater • Pulmonary artery reactivity upon challenge with pulmonary vasodilator • Lung biopsy evidence of reversibility to pulmonary arterial changes
Interventional Options: • Percutaneous closure procedure of choice when appropriate • Similar indications for closure as discussed • Only available for Secundum ASD with stretched diameter < 41 mm • Need adequate rims to enable secure device deployment • Cannot have anomalous pulm venous connection, be too proximal to AV valves, coronary sinus, or systemic venous drainage
Percutaneous Closure: • Amplatzer device • Introduced by AGA Medical in 1996 • Nitinol wire mesh with middle “waist” • Amplatzer septal occluder • Single defects • Amplatzer fenestrated septal occluder (“Cribiform”) • Multiple hole ASD • Thinner central waist
Role of echo in percutaneous closure: • TEE used in past, but requires general anesthesia • Intracardiac echo: • Mullen et al, JACC 2003 • Feasability and accuracy of ICE in guiding percutaneous closure of ASDs • Prospective study of 24 pts; using ICE as primary imaging modality • Close agreement to TEE • Successful guidance in 96% of cases • Identify residual shunts in 98% of cases • Detected 100% of adverse events
Evaluation by Echo post-closure: • Assess residual shunting/flow • Assess for complications • Follow-up ventricular function
Complications/ Results: • < 1% of cases with complications • Includes device embolization, atrial perforation, thrombus formation • Clinical closure achieved in > 80% of cases • Improves functional status and exercise capacity
Early and Intermediate Follow-up: • Medical management: • ASA • Bacterial endocarditis prophylaxis x 6 months • F/U Echo 1 year (after immediate post study done to confirm success) • Device vs Surgery: • Overall similar costs and success/safety • Likely due to expense of device • Shorter hospital course with device
Surgical Treatment: • Reserved for cases that are not candidates for percutaneous closures: • Non-secundum ASDs • Secundum ASDs with unsuitable anatomy • Primary suture vs tissue/synthetic patch • Symptomatic improvement seen • Does not prevent AF/aflutter in adults (especially >40 years old) • Concomitant MAZE a consideration