Download
1 / 40
400 likes | 737 Views
Developing Acute Stroke Services Diagnosing Screening Acute Care pathways Thrombolysis Dr C. Roffe Clinical Lead Shropshire and Staffordshire Heart and Stroke Network . Patient or bystander recognizes stroke. Dial 999. Ambulance response Blue-light FAST positive potential strokes to A&E.

E N D
Developing Acute Stroke ServicesDiagnosingScreeningAcute Care pathwaysThrombolysisDr C. RoffeClinical Lead Shropshire and Staffordshire Heart and Stroke Network
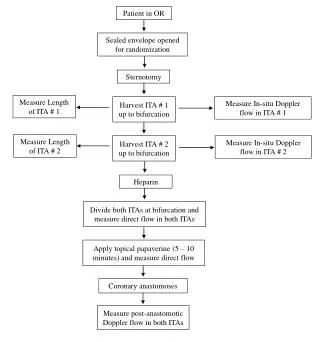
Patient or bystander recognizes stroke Dial 999 Ambulance response Blue-light FAST positive potential strokes to A&E Fits thrombolysis criteria pre alert A&E Does not fit thrombolysis criteria Immediate assessment Thrombolysis pathway and CT within 15 min Stroke pathway and CT within 1 hour Thrombolysis Admit to ASU within 4 h of presentation
F A S T Face–Arm–Speech Test F Facial weakness: Can the person smile? Has their mouth or an eye drooped? A Arm weakness: Can the person raise both arms? S Speech problems: Can the person speak clearly and understand what you say? T Time to call 999.
ROSIERRecognizing Stroke in the Emergency Room Only count new symptoms Exclude hypo by BM stix Unilateral facial weakness? y (1) n (0)Unilateral arm weakness? y (1) n (0) Unilateral leg weakness? y (1) n (0) Speech disturbance ? y (1) n (0) Visual field defect? y (1) n (0) Any loss of consciousness or syncope y (-1) n (0) Any seizures? y (-1) n (0) Rosier >0 suggests ischaemic stroke and potential thrombolysis case
Stroke or TIA? • Symptoms still present => Stroke • Symptoms gone =>TIA
WHO DEFINITION OF STROKE A NEUROLOGICAL DEFICIT OF • Sudden onset • With focal rather than global dysfunction • In which, after adequate investigations, symptoms are presumed to be of non-traumatic vascular origin • and last for >24 hours
Stroke onset • Witness? • Woke with hemiparesis? • Found collapsed? • Sudden/gradual/ stuttering
ABCD2 Scoring for all new TIAs Stroke risk within 1 week 6% for scores 4-5, 12% for scores >5 Admit all with score 5 or above.
TIA management • Do not allow any TIA patient to leave the department without having administered the first dose of antiplatelet • ABCD 4 or above admit or ensure TIA clinic appointment (and Doppler) within 24 hours. • Endarterectomy within 48 h for patients with symptomatic stenosis • ABCD <4 see in TIA clinic within 1 week. Endarterectomy within 14 days for patients with symptomatic stenosis This will reduce strokes within 1 week by 80%!!!
Role of Paramedics • Establish working diagnosis of stroke/TIA • Identify potential thrombolysis candidates • Prealert A&E if thrombolysis an option • Establish onset time • Bring a witness • Airway Breathing Circulation • Exclude Hypo BM • Prevent aspiration • Get patient to nearest hyper acute stroke centre
CT Head scan • Intracerebral haemorrhage • Correct abnormal INR or low platelets immediately • Neurosurgical referral • Cerebral Infarct • Thrombolysis or • immediate antiplatelet treatment
Early signs of infarctionLoss of insular ribbon 14.jpg SW, day 1
Other tests • FBC • U&E • INR • Glucose • ECG • Carotid Doppler
DH A New Ambition for StrokeA consultation document for a National Stroke strategy Dec 2008 If 10% of stroke patients in the UK were given thrombolysis, 1000 people less would be dead or dependent in one year. http://www.dh.gov.uk/en/Publicationsandstatistics/Publications/PublicationsPolicyAndGuidance/DH_081062
NINDS trial of rt-PA for acute ischaemic stroke • 633 patients recruited • Rt-PA 0.9 mg/kg (10% bolus the rest over 1 h) given within 3 hrs of symptom onset • BP<185/110 • Not on warfarin or heparin, platelets and coagulation normal • Blood glucose 2.7-22 mmol/L • No seizure at onset Quasi intensive care environment Aggressive BP control 16,000 screened to recruit 633 N Engl J Med 1995;333:1581-1587.
NINDS rt-PA trial 1995Improvements in dependency (modified Rankin Scale: mRS) Mean Score 2.8 for rt-PA and 3.3 for control : difference 0.5 mRS points* Number needed to treat to improve by 1 point is 2* Number needed to treat to improve by 1 or more points is 3** Number needed to treat to make one patient more independent =5* Needs No help Wheelchair Dead Normal INDEPENDENT DEPENDENT * My own calculation bases on the original paper ** Saver. Arch Neurol, Jul 2004; 61: 1066 - 1070.
Eligibility • Age 80 or below • Previously fit and independent • Onset time known and less than 3 hours • CT excludes haemorrhage
Exclusions • Recent surgery, biopsies arterial cannulation • Increased bleeding risk • Past history of intracranial haemorrhage • Any CNS pathology other than current stroke • Any past stroke plus diabetes • Stroke within 3 months • Systolic blood pressure >185
Alteplase (rt-Pa) • 0.9 mg/kg body weight • 10% as bolus over 2 min • 90% as infusion over 1 hour No heparin for 24 hours
Post thrombolysis Care • Needs trained team / ASU • Neurological observations (NIHSS) • Blood pressure • Observation for complications • Scan at 24 h • Prevent recurrence • Early Doppler/ CTangio in recovered cases
The acute stroke pathwayHow can I make sure my patient will do well?
Most complications of stroke develop in the first 24 hours Management in the first few hours has a major effect on outcome and LOS
Important factors for successful early stroke rehabilitation • Mobilise ASAP The probability of returning home decreases by 20% for each day the patient is not mobilized • Maintain normal haemodynamic and biochemical environment • Prevent complications • Keep patient and family informed
2. Prevent Aspiration • Swallow screen on arrival on ASU • Sit up • Drowsy patients in recovery position • Antiememtics for haemorrhages and patients who feel sick • All members of staff have at least basic knowledge of the diagnosis and management of swallowing problems
3. Prevent hypotension and dehydration • IV saline • Sufficient fluids by mouth or ngt
4. Prevent pneumonia Mobilization
Mouthcare Dysphagic patients have impaired oral movements resulting in debris, pooled secretions and tongue coating.
5. Prevent hospital acquired infectionsMRSA/ ESBL/ C.Difficile Avoid catheters at all costs Hand hygiene Bed spacing Appropriate antibiotics
7. Prevent stagnation and deterioration • Time does not cure strokes • Give at least 45 min of each therapy needed every day 7/7
7. Detect and treat problems early • 72 hour monitoring • Neurological scores (NIHSS/SSS) • Daily consultant ward rounds 7/7