Download
1 / 16
170 likes | 199 Views
Explore Duke's journey to improve the quality of research and trials through its Translational Medicine Quality Framework. Uncover the challenges faced, the committee's recommendations, and the external review process. Engage in the ongoing conversation about enhancing medical research quality.

E N D
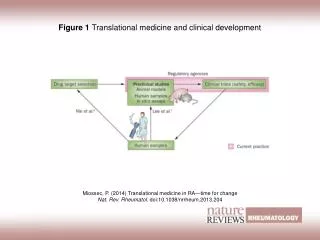
Translational Medicine Quality Framework for Duke Medicine March, 2011
Translational Medicine Quality Framework • This past year Duke became the center of a national controversy concerning the use of gene expression data as the basis for clinical trials. • Questions were raised about the veracity of the data and the quality of the analyses from one of our laboratories. • These laboratory findings were rapidly translated into decision support instruments for use in human clinical trials.
TMQF Background • As the public record now shows, the work of our investigators was flawed and thus did not demonstrate that personalized genomic predictors could be used for creating “tailored” cancer care. • Problems with data provenance, unexplained errors related to data management, and implausible data combinations that escaped detection at two different levels of independent peer review nullified the work and led to the trials being closed.
TMQF Committee Formation and Charge • Duke Chancellor for Health Affairs Victor Dzau, MD, convened an internal Duke committee to review institutional approaches to assure the quality of discovery science destined for clinical application. • A panel of external experts was also convened to review the recommendations of the TMQF Committee. • The report is now available at http://medschool.duke.edu/modules/som_research/index.php?id=22. • Faculty and staff comments are welcome at tmqffeedback@duke.edu
TMQF Committee Chair: Robert M. Califf, MD • Donald F. Fortin, MD, Professor of Cardiology • Vice Chancellor for Clinical Research • Director, Duke Translational Medicine Institute Co-Chair: Sally Kornbluth, PhD • James B. Duke Professor, Department of Pharmacology and Cancer Biology • Vice Dean for Research, Duke University School of Medicine Faculty Membership Michael Cuffe, MD, MBA • Vice President for Medical Affairs, Duke University Health System • Vice Dean for Medical Affairs, Duke University School of Medicine Elizabeth R. DeLong, PhD • Professor and Chair, Department of Biostatistics and Bioinformatics • Co-Director, Outcomes Research & Assessment Group, Duke Clinical Research Institute Henry S. Friedman, MD • James B. Powell, Jr., Professor of Neuro-Oncology and Professor of Pediatrics • Deputy Director, Preston Robert Tisch Brain Tumor Center Geoffrey S. Ginsburg, MD, PhD • Professor of Medicine and Pathology • Director, Center for Genomic Medicine, Duke Institute for Genome Sciences & Policy David B. Goldstein, PhD • Richard and Pat Johnson Distinguished University Professor • Professor of Molecular Genetics and Microbiology, and Biology • Director, Duke Center for Human Genome Variation Robert A. Harrington, MD • Richard Stack, MD/Guidant Foundation Professor of Cardiology • Professor of Medicine, Cardiology • Director, Duke Clinical Research Institute
TMQF Committee Elizabeth R. Hauser, PhD • Professor and Chief, Division of Medical Genetics, Department of Medicine • Director, Duke Center for Human Genetics Barton F. Haynes, MD • Frederic M. Hanes Professor of Medicine and Immunology • Director, Duke Human Vaccine Institute Mary E. Klotman, MD • Professor and Chair, Department of Medicine Robert J. Lefkowitz, MD • James B. Duke Professor of Medicine and Professor of Biochemistry H. Kim Lyerly, MD • George Barth Geller Professor of Research in Cancer • Director, Duke ComprehensiveCancer Center Ross E. McKinney, Jr., MD • Professor of Pediatrics • Director, Trent Center for Bioethics, Humanities, and History of Medicine Anthony R. Means, PhD • Nanaline H. Duke Professor and Chair, Department of Pharmacology and Cancer Biology • Professor of Medicine • Co-Director, Duke Cancer Institute Christopher B. Newgard, PhD • W. David and Sarah W. Stedman Distinguished Professor • Professor of Pharmacology and Cancer Biology, Biochemistry and Internal Medicine • Director, Sarah W. Stedman Nutrition and Metabolism Center Bruce A. Sullenger, PhD • Joseph and Dorothy Beard Professor, Department of Surgery • Director, Duke Translational Research Institute Christopher G. Willett, MD • Professor and Chair, Department of Radiation Oncology • Co-Director, Duke Cancer Institute Jo Rae Wright, PhD • Professor of Cell Biology • Dean of the Graduate School and Vice Provost, Duke University
TMQF External Review Panel Eugene Braunwald, MD • Distinguished Hersey Professor of Medicine • Harvard Medical School • Brigham and Women's Hospital David L. DeMets, PhD • Professor, Biostatistics and Medical Informatics • University of Wisconsin David Ginsburg, MD • James V. Neel Distinguished University Professor of Internal Medicine and Human Genetics • Warner-Lambert/Parke-Davis Professor of Medicine • Investigator, Howard Hughes Medical Institute • University of Michigan Xihong Lin, PhD • Professor of Biostatistics • Coordinating Director, Program of Quantitative Genomics • Harvard School of Public Health Jeffrey M. Trent, PhD • President and Research Director • Translational Genomics Research Institute (TGen) • Senior Investigator, Genetic Basis of Human Disease Division • Head, Melanoma Therapeutics Lab Elias A. Zerhouni, MD • President, Global Research and Development • Sanofi-Aventis
TMQF CommitteeStaff Ann E. Bradley, BS, BA, JD • Associate University Counsel, Office of Counsel • Duke University/Duke University Health System Paul P. Lee, MD, JD • James P. Gills, III, MD and Joy Gills Professor of Ophthalmology • Senior Advisor to the Chancellor and • Director, Applied Health Systems Research, Duke University Health System • ViceChairman, Duke Eye Center JonathanMcCall • Senior Editor, Writing Services • Communications Group, Duke Clinical Research Institute Deborah A. Roth, MS • Associate Dean for Clinical Research Administration, School of Medicine • Chief Operating Officer, Duke Translational Medicine Institute
Landscape of Research • Basic science has been advanced by focusing on independent work of individuals and small teams. • Theories and concepts evolve through serial hypothesis testing and replication/refutation by independent laboratories. • In the past, the route from a basic discovery to clinical application was long, with many steps in which different people could test concepts.
Current Landscape • Systems biology is evolving as a concept. • Requires multidisciplinary teams • Complex data sets and multiple measures • The route from discovery to human application is becoming shorter due to increasing discovery research with human samples and tissues. • Administrative structures of academic health and science systems are more complex.
Recommendation 1: Data Provenance Prior to application of research to humans in a manner that directs diagnostic testing or therapy either in clinical studies or in commercialization, findings must be reproducible (both internally and externally) based on additional documented data sets. Documentation of internal reproducibility should extend in a readily traceable manner back to the fundamental source of the original data, a concept known as data provenance. External reproducibility should be demonstrated in data external to those used to produce the original findings. Optimally, this could include a requirement that the data analysis be reproduced in an independent facility in addition to being replicated in second data sets.
Recommendation 2: The Imperative to Include Adequate Quantitative Expertise Scientific studies must be conducted with adequate quantitative expertise, applied under proper standards to the design, conduct, analysis, and presentation of results.
Recommendation 3:Accountability for Quality Governance and oversight of science with direct implications for patient care can no longer be seen as residing solely within the purview of any one laboratory. Given consideration of public investment, public trust, and direct impact on the wellbeing of patients, a chain of accountability extending beyond the individual laboratory to scientific leaders at local and institutional levels must be established.
Recommendation 4: Special Review of Conflicted Research In the specific case of diagnostic or prognostic tests developed within the institution for which financial gain for scientists and/or the institution is possible or other forms of conflict are evident, a panel of independent experts should be convened to review the science underlying the test before the test is used in human studies or licensed.
Conclusions of the TMQF Committee • This is only the beginning of what we believe will be a constantly evolving scientific framework, one characterized by increasing transparency and global sharing to produce new knowledge at accelerating rates • Understanding that data provenance, quantitative expertise, accountability, use of genomic tools by scientists with deep understanding of the underlying biology, and external review are all critical elements of this process should improve the capacity to move from discovery to improved human health. • We are equally convinced that shortcuts or lack of attention to the checks and balances noted in this report would be detrimental and even potentially damaging, especially in research involving human research participants. • We will endeavor to work collaboratively with leading institutions to implement these ideas (and better ideas as they evolve) in an efficient manner that encourages new advances among the community of scientists and practitioners.
Plans for Implementation • After a 1-month period for input from faculty and staff, the TMQF document will be finalized. • In parallel, an Implementation Plan is being developed by the TMQF Committee. • The Implementation Plan will require: • A determined effort to foster an institutional culture in which dissenting opinions and critical evaluation of colleagues are encouraged; and • An investment in critical infrastructure support.