Download
1 / 86
860 likes | 987 Views
ANEMIAS Mohammad Abu-Fara. MD. ANEMIA. Anemia : Is defined as a reduction in one or more of major RBC measurements. HGB. HTC. RBC count . Anemia is not a disease by itself but is one of the major signs of disease.

E N D
ANEMIAS Mohammad Abu-Fara. MD
ANEMIA Anemia: Is defined as a reduction in one or more of major RBC measurements. HGB. HTC. RBC count . Anemia is not a disease by itself but is one of the major signs of disease. May be the first manifestation of a systemic disease, along with other nonspecific complaints such as fever, weight loss, anorexia.
HGB Concentration: measures the major oxygen-carrying pigment in whole blood. Values are expressed as grams of HGB per dL of whole blood (g/dL). The normal ranges for HB. Varies in men and women and in different age group. Normal range: M 13-16,5 g/dL F 12-15,5 g/dL
Hematocrit (HTC): Is the percent of a volume of whole blood occupied by intact RBCs. Values are expressed as a percentage. Normal range: M 41-51%. F 37-47%.
RBC Count: Is the number of RBCs contained in a unit of whole blood. Values are expressed as millions of cells per uL of whole blood. Normal range: M 4,5-6,5 F 3,8-5,8
VOLUME STATUS The three measurements are all concentrations. As such they are dependent upon both the RBC mass and the plasma volume. 1.In acute bleeding anemia develops only after 36-48 hours. 2.Pregnancy:RBC mass is increased by 25% and plasma is increased by 50%.Normal values in pregnancy are different. 3.Dehydration.
SPECIAL POPULATIONS 1.Living at high altitude. 2.Smoking and air pollution. 3.African-Americans—lower values. 4.Populations with a high incidence of ch. diseases. 5.Athletes. 6.The elderly: should not have a lower normal range for fear of missing a serious underlying disorder.
ERYTHROPOESIS The rate of RBC production equals the rate of RBC destruction. Approximately 1% of RBCs is removed from the circulation daily. The rate of RBC production can increase markedly under the influence of high levels of EPO.5-7 folds.
CLINICAL CONSEQUENCES OF ANEMIA The signs and symptoms induced by anemia are dependent upon the degree of anemia as well as the rate at which the anemia has evolved. Symptoms of anemia can result from two factors: 1.Decreased O2 delivery to tissues. 2.Hypovolemia/acute blood. loss/.
COMPENSATORY MECHANISMS Signs and symptoms depend also on the compensatory mechanisms. 1.Extraction of O2 by the tissues can increase from 25% to 60%. 2.Cardiac compensation :stroke volume and heart rate/cardiac output/. Thus normal O2 delivery can be maintained by 1 and 2 at rest at HBG as low as 5g/dL,assuming that the intravascular. volume is maintained. Thus symptoms will develop when HBG falls below this level at rest or at higher HBG during exertion or when cardiac compensation is impaired.
SYMPTOM AND SIGNS Symptom :is a sensation or change in health function experienced by the patient. It is a subjective report. . Dyspnea /S.O.B. :on exertion/at rest. Fatigue/tiredness. Signs and symptoms of hyperkinetic state: 1.bounding pulses. 2.palpitations. 3.roaring in ears.
In more severe anemia: Lethargy, confusion, CHF, angina, MI., Pallor. Headache. Visual impairment, syncope Complications of extra cellular volume depletion/in acute bleeding/ Symptoms and sign due to the underlying cause of anemia .
Iron deficiency • Most cases are caused by menstrual loss and increased iron requirements of pregnancy. • GI bleeding is the presumed etiology in most patient • Decreased iron absorption (celiac disease, postgastrectomy, or increase iron requirement as in lactation. • History of pica (consmption of substances such as ice, starsh or clay ) can be obtained . • Signs : splenomegaly, kiolonychia (spoon nail ) and plummer- vinson syndrome (glossitis, dysphagia, and esophageal webs) are rare finding.
Vitamin B12 and Folate deficiency Glossitis, angular stomatitis, juandice, splenomegaly and neurological syndrome of pernicious anemia ( subacute combined degeneration-demylination of dorsal and lateral columns of spinal cord. unsteady gait and progress to irreversible damage and bladder disturbance (only in VB12 def.)
Sign: is an objective evidence of the presence of a disease or disorder .Signs are discovered and reported by the physician, not by the patient. Elevated BP. Skin rash. Tachypnea.
CAUSES OF ANEMIA There are 2 interrelated approaches one can use to help identify the cause of anemia. 1.Kinetic approach. 2.Morphologic approach.
KINETIC APPROACH Anemia can be caused by one or more of 3 independent mechanisms. 1.Decreased RBC production. 2.Increased RBC destruction. 3.RBC loss.
MORPHOLOGIC APPROACH According to RBC size. Mean Corpuscular Volume /MCV/. RBC size/MCV/ is 80-96 femtoliters(fL). Microcyte. Macrocyte. Normocyte.
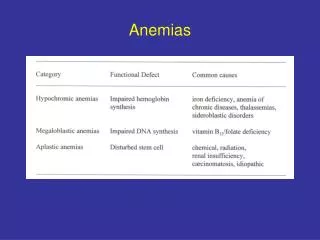
ANEMIAS ACCORDING TO THE RBC SIZE 1.Microcytic anemia. 2.Macrocytic anemia. 3.Normocytic anemia.
MICROCYTIC ANEMIAS Are associated with an MCV below 80 fL. IDA ACD Thalassemias.
MACROCYTIC ANEMIAS Are characterized by an MCV above 100 fL. Reticulocytosis. Vit.B12 def. Folate def. MDS. Liver disease Hypothyroidism
NORMOCYTIC ANEMIAS By definition the MCV is normal. ACD. MDS.
EVALUATION OF THE PATIENT WITH ANEMIA-1 • Anemia is one of the major signs of disease. • It is never normal and it's cause should be always be sought. • History. • Physical examination. • Simple lab. tests. Are all useful in evaluating the anemic patient.
EVALUATION OF THE ANEMIC PATIENT-2 The workup should be directed towards answering the following questions: 1.Is the patient bleeding (now or in the past) ?. 2.Is there evidence of increased RBC destruction? 3.Is the BM suppressed?. 4.Is the patient iron deficient?if so,why?.
Anemia associated with red blood cell loss or destruction • Sickle cell disease • G6PD deficiency • Hemolytic anemia
HEMOSTASIS-1 • In health hemostasis ensures that the blood remains fluid and contained in the vascular system. • If a vessel wall is damaged,a number of mechanisms are activated promptly to limit bleeding, involving 1-Endothelial cells. 2-Plasma coagulation factors. 3-Platelets. 4-Fibrinolytic system.
HEMOASTASIS-2 • These activities are finely balanced between keeping the blood fluid and preventing intravascular thrombosis. 1-Pimary hemostasis: immediate but temporary response to vessel injury . Platelets and von willebrand interact to form a primary plug , after which platelet activation occurs and blood vessels constrict, limiting flow. 2-Secondary hemostasis: (coagulation) :is slower process that results in the formation of a fibrin clot .
Coagulation is initiated when vascular damage exposes extravascular tissue factor initiating activation of factor V11, factor X and prothrombin with subsequent activation of factor V,V111,1X,X1,and X111,leading to accelerated and sustained generation of fibrinogen to fibrin and formation of durable clot. 3-Fibrinolysis: activation of fibrin-bound plasminogen resulting in clot lysis.
ROLE OF ENDOTHELIAL CELLS IN HEMOSTASIS • Blood vessels are lined with endothelial cells,which synthesize and secrete various agents,that regulate hemostasis. 1-Procoagulant(prothrombotic) agents: tissue factor, von Willebrand factor, F V ,F VIII. 2-Anticoagulant(antithrombotic) agents: prostacyclin,Nitric oxide,endothelin-1.
ROLE OF PLATELETS IN HEMOSTASIS • Each megacaryocyte produces 1000-2000 platelets,which • remain in the circulation for about 10 days. • Releasing of hemostatic proteins. • Platelet adhesion. • Platelet aggregation.
COAGULATION SYSTEM • Coagulation factors: are plasma proteins synthesized in the liver which ,when activated lead to the deposition of fibrin. 1-Initiation phase: leads to the formation of the complex TF-VIIa. 2-Amplification phase: leads to the formation of a small amount of thrombin from prothrombin. 3-Propagation phase: leads to the formation of much larger amounts of fibrin.
INHIBITORS OF COAGULATION Are proteins that inhibit activated procaogulation enzymes and prevent excessive intravascular coagulation Raised levels are not associated with bleeding. Reduced levels may predispose to thrombosis. Antithrombin. Protein C, Protein S. Tissue Factor Pathway Inhibitor (TFPI).
FIBRINOLYSIS • Small amouns of fibrin are constantly deposited within the vascular system and are removed by the fibrinolytic system Plasminogen Plasmin Fibrin FDPs
ASSESSMENT OF BLEEDING SYMPTOMS 1-Careful and full clinical history and examination. (determining whether a bleeding is present or likely congenital or acquired, mild or severe and involving primary or secondary hemostasis ) 2-Appropriate lab. investigations. 3-Other investigations.
HISTORY • 1-Site of bleeding( dental extractions, circumcision, menstration, labor or delivery and trauma or surgery. Or easy bruising • 2-Duration of bleeding and severity. • 3-Precipitating cause. • 4-Surgery. • 5-Family history. • 6-Systemic illnesses (acquired bleeding disorders). • 7-Drugs.
Clinical Features of Bleeding Disorders Platelet Coagulation disorders factor disorders Site of bleeding Skin Deep in soft tissues Mucous membranes (joints, muscles) (epistaxis, gum, vaginal, GI tract) Petechiae Yes No Ecchymoses (“bruises”) Small, superficial Large, deep Hemarthrosis / muscle bleeding Extremely rare Common Bleeding after cuts & scratches Yes No Bleeding after surgery or trauma Immediate, Delayed (1-2 days), usually mild often severe
LABORATORY STUDIES • Initial studies should include a platelet count, prothrombin time (Pt ), activated partial thromboplastic time (aPtt) and peripheral blood smear review. • platelet count low : manual slide review to rule out a platelet clumping artifact. • Bleeding time (BT) : may detect quantitative or qualitative disorder of platelets or vWF or abnormalities of capillary integrity. • prolonged after medication as aspirin.
In vitro platelet aggregation • Von Willebrand factor antigen • von Willebrand factor activity , ristocetin cofactor (vWF :RCo ) • Von Willbrand factor multimer analysis.
Secondary hemostasis • Prothrombin time (Pt) : extrinsic pathway (factor V11,and common pathway factor X,V ,prothrombin ) coagulation factors and fibrinogen. • INR : (patient PT/ mean normal PT)ISI • Activated partial thromboplastin times (aPTT): intrinsic pathway (kininogen, prekallikrein, factor X11, factor 1X,factor X1 and factor V111) and common pathway (factor V,facter X ,prothrombin and fibrinogen. • Thrombin time (TT) • Fibrinogin • Clot urea stability • Mixing studies coagulation plasma activity .
Inherited bleeding disorders Hemophilia A and B Von Willebrand disease Other factor deficiencies Acquired bleeding disorders Liver disease Vitamin K deficiency/warfarin overdose DIC Coagulation factor disorders
Hemophilia A and B Hemophilia A Hemophilia B Coagulation factor deficiency Factor VIII Factor IX Inheritance X-linked X-linked recessive recessive Incidence 1/10,000 males 1/50,000 males Severity Related to factor level <1% - Severe - spontaneous bleeding 1-5% - Moderate - bleeding with mild injury 5-25% - Mild - bleeding with surgery or trauma Complications Soft tissue bleeding
Hemophilia Clinical manifestations (hemophilia A & B are indistinguishable) Hemarthrosis (most common) Fixed joints Soft tissue hematomas (e.g., muscle) Muscle atrophy Shortened tendons Other sites of bleeding Urinary tract CNS, neck (may be life-threatening) Prolonged bleeding after surgery or dental extractions
Treatment of hemophilia A • Intermediate purity plasma products • Virucidally treated • May contain von Willebrand factor • High purity (monoclonal) plasma products • Virucidally treated • No functional von Willebrand factor • Recombinant factor VIII • Virus free/No apparent risk • No functional von Willebrand factor
Dosing guidelines for hemophilia A • Mild bleeding • Target: 30% dosing q8-12h; 1-2 days (15U/kg) • Hemarthrosis, oropharyngeal or dental, epistaxis, hematuria • Major bleeding • Target: 80-100% q8-12h; 7-14 days (50U/kg) • CNS trauma, hemorrhage, lumbar puncture • Surgery • Retroperitoneal hemorrhage • GI bleeding • Adjunctive therapy • Tranexemic acid or DDAVP (for mild disease only)
Complications of therapy • Formation of inhibitors (antibodies) • 10-15% of severe hemophilia A patients • 1-2% of severe hemophilia B patients • Viral infections • Hepatitis B Human parvovirus • Hepatitis C Hepatitis A • HIV Other
Treatment of hemophilia B • Agent • High purity factor IX • Recombinant human factor IX • Dose • Initial dose: 100U/kg • Subsequent: 50U/kg every 24 hours
von Willebrand Disease: Clinical Features • von Willebrand factor • Synthesis in endothelium and megakaryocytes • Forms large multimer • Carrier of factor VIII • Anchors platelets to sub endothelium • Bridge between platelets • Inheritance - autosomal dominant • Incidence - 1/10,000 • Clinical features - mucocutaneous bleeding