Anemias
E N D
Presentation Transcript
Anemias 中国医科大学附属第一医院血液科 李艳
CUF-S (造血干C、红系祖C)↓ proerythroblast (原始RBC)↓ Basophilic normoblast ( 早幼RBC)↓ Polychromatic mormoblast(中幼RBC)↓ Orthrochromatic normoblast (晚幼RBC)此阶段脱核进入血循环↓ Reticulocyte (网织RBC)经特殊染色见到丝状或网状结构, 保留残余线粒体和核糖,仍有继续合成Hb的能力(从早幼RBC开始)↓erythrocyte
Definition • A reduction below normal in theconcentration of hemoglobin , the mass of red blood cells and/or the hematocrit in the blood. In men Hb < 120g/L RBC <4.5×1012/L HCT <0.42 In women Hb < 110g/L RBC<4.0 ×1012/L HCT<0.37
Factors influencing Hb concentration Sex Age Altitude Alterations in plasma volume
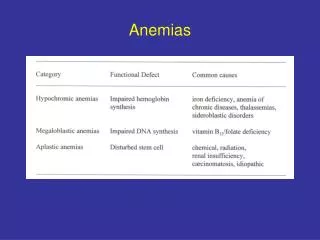
★Classification Morphologic classification
Kinetic classification(Classified according to etiology and pathogenesis) 一、Decreased erythropoiesis Proliferation and differentiation abnormalities of SC HSC: AA, Fanconis anemia, MDS Erythrocytic progenitors : Pure red cell aplasia, Anemias caused by kidney failure and endocrine disorders
Marrow infiltrationleukemiascarcinomamultiple myeloma myelofibrosisMalignant histocytosis
Production and maturation blockages of differentiating cells DNA synthesis blockage : Vit B12, falic acid difficiencies, 嘌呤和嘧啶 metabolic defects→Megaloblastic anemiaHb synthesis blockage : Heme production defect : IDA Heptoglobin production defect : Thalassemias
4 Unknown reason or several mechanisms Sideroblastic anemiaChronic disease anemias (chronic inflummation, infections, 尿毒症, Hepatic disorders, neoplasm, connective tissue disease, endocrine disorders)
二、Accelerated destruction of red cells 1)Endogenous (intra-erythrocyte defects) 1.Membrane defects of erythrocytes : Hereditary :Hereditary spherocytosis (HS) Hereditasy elliplocytosis (HE) Acquired : PNH2.Enzyme defects Glucose--6--Phosphate Dehydrogenase (G6PD) deficiency Pyruvate kinase deficiency 3.Abnormal haptogllbin synthesis : Sickle cell anemia, Hemoglobinopathies Thalassemias
2)Extragenous Immune HA : AIHA, neonatal HA,mismatched transfusion,drug-induced HA 2. Mechanical : march hemoglobinuria , cardiac valves prostheses, microangiopathic hemolytic disorders. 3.Due to chemical, physical or microrganisms : Chemical toxin-and drug-induced hemolysis,large scale burned patient (severe burned patient)Infection-induced , benzene, radiation microrganisms: Malaria, virus, etc. 4. Increased damage of monocyte-macrocyte system : Hypersplenism
三. Blood loss ◆Acute posthemorrage anemia ◆Chronic bleeding →IDA
Classified accordind to the proliferative situations of BM Hyperplastic anemias (增生性贫血):Hemolytic anemia Anemia caused by blood loss Megaloblastic anemia, IDA Hypoplastic anemias (增生减低性贫血): AA
Clinical manifestations Factors influencing symptoms:Severity of anemia Hb<80~90g/L→symptoms Rapidity of anemia Abrupt loss of 20% of the circulating blood volume → marked pallor, postural hypotension and tachycardia (心动过速)The loss of 50% → severe shock even dealth.
In contrast, the gradual loss (even Hb 30~40g/L) of the circulating red cell mass in a patient with pernicious anemia may occur without any symptoms at all.
Why? • Red cell 2, 3 DPG (RBC内2, 3-二磷酸甘油酸)↑ In anemia the oxyhemoglobin dissociation curve usually shifts (右移) in a manner to increase the quantity of oxygen released in tissues without oppeciably altering the quantity of osygen bound in the lungs. Red cell 2,3 diphophoglycerate (2,3 DPG) regularly increases in anemic patients to mediate this effect. Maximum elevation of RBC 2,3 DPG increases oxygen delivery only about 30 per cent , but this is a highly efficient form of compensation requiring no significant expenditure of energy.
The aged patients or patients with vascular or cardiac diseases may not stand to milder anemia.
The level of anemia at which symptoms occur is highly variable among individuals as would be expected from the widely differing degrees of physical activity , physical conditioning , circulatory adequacy , and sensitivity or stoicism of the population.
1.General manifestations:(Nonspecific and reflect tissue hypoxia)Tiredness, fatigue→ the most common, the earliest symptom Pallor of skin and mucosa→sharedchracteristic2.Cardiovascular systems :Palpitations and dyspnea on exertion,breathlessness→common symptomsValvulae murmurs Hb <30g/L, >3m→Anemic cardic disease
3. Neurologic system :Headache, Dizziness, Confusion, decreased mental acuity (记忆力衰退), 晕厥,注意力不集中,失眠,耳鸣.severe anemia→Coma4 .Digestive system:Anorexia (食欲不振),厌食→early megaloblastic anemia Nausea(恶心),flatulence(胀气),diarrhoea(腹泻) or constipation (便秘)lingual abnormalities (舌的改变):common
5.Genitourinary system:severe anemia→ polyurea (多尿), hypobaric urine (尿比重低), proteinuria (蛋白尿): 肾小球滤过功能和小管分泌及回收功能障碍female:disturbed menstruation (月经紊乱), 性功能减退多见6.Other:7. Manifestations of underlying disease:
The process of correct diagnosis is the one of differential diagnosis.Steps:1. To Establish the type of anemia2. To find out the cause or underlying diseases of anemia Diagnosis
Cause or inducer of anemia:Nutrition, special habits for food change in stool habits: stool Guaiacs in all professioninfluation of surrounding environment chronic diseases menstruation, marriage 一.History
2. Developing processes, severity & complications of anemiasDuration and onset of symptoms3.Important laboratory results, diagnosis, treatments and their effects.
skin and mucosa: pallor, jaundice, petechiaehair and nails adenopathy (淋巴结肿大) hepatomegaly-splenomegalyneurologic abnormalities 肛门及妇科盆腔检查 二.Physical examination
1、The hemogram (血像) Routine blood exam(Hb,RBC)The reticulocyte count (RC) RC↑:hyperplastic RC↓:hypoplastic 三、Laboratory findings
Reticulocyte Count • Normal: 0.002-0.015 • Is required in the evaluation of all patients with anemia as it is a simple measure of production • Young RBC that still contains a small amount of RNA • Normally take 1 day for reticulocyte to mature. Under influence of epo takes 2-3 days • 1/120th of RBC normally
Absolute Retic count • Retic counts are reported as a percentage: RBC count x Retic % = Absoulte retic count normal: (77+23) x 109/L • Absolute Retic counts need to be corrected for early release ( If polychromasia is present) • Absolute retic/2 (for hct in mid 20’s) • Absolute retic/3 (hct <20)
MCV(the mean corpuscular volume): the most useful of the RBC indices.MCH,MCHC: are rarely as helpful as the MCVThe leukocyte and platelet count: Anemia with a diminished leukocyteand platelet count-pancytopenia-suggests either primary marrow disease, megaloblastic anemia, or hypersplenism.Examination of the peripheral blood smear:
2. Examination of bone marrow 骨髓涂片检查:主要观察BM增生程度,各系统细胞分类计数,异常细胞,正常BM组织有核细胞与脂肪组织各占1/2,前者增多(尤其是红系)见于增生性贫血,后者增多代表BM增生低下,见于AA,骨髓小粒是血液稀释与否的一个重要标志。Examination of aspirated smears in general gives superior cytologic information while the core biopsy provides crucial information concerning the overall cellularity, as well as the presence of fibrosis, tumor, or granulomas. Both procedures are complemantary and are best performed together when the diagnosis is in doubt. Bone marrow iron staining
3. Some useful ancillary tests 1) Stools for occult blood 2) Tests for hemolytic anemia such as Coombs’test 3) Tests for nutritional anemia such as serum folic acid, serum Vitamin B12, SI, SF, etc. 4) Liver and kidney function tests 5) Immunologic tests 6) 影像学检查:钡餐透视,钡灌肠
Treatment 一、 Treatment of the causes The purpose is the treatment of the underlying disease. Gastric cancer→Pernicious anemia(恶性贫血) (megaloblastic anemia)
二、Drugs 明确病因之前且忌乱投药 • Iron agents; calculation of dose • falic acid , Vit B12 • Vit B6 • Corticosteroids : AIHA,AA, PNH • Androgens: may promate reythropoiesis: 1.)刺激EPO分泌。2)增强BM对EPO的效应。 • EPO: Anemia caused by kidney diseases • Immunosuppression agentsALG (antilymphocyte globulin)CsA: Acute and severe AA
三、 Transfusions Avoid of complications as hepatitis and AIDS • Whole blood • Frozed red cells • Washed red cells • Leukocyte poor packed cells (浓缩RBC) Chronic anemia : Hb<60g/L→Transfusion
Hereditary spherocytosisAIHAHypersplenism由于胸腺瘤(Thymoma)引起的纯红AA,切除胸腺可使部分患者病情缓解。 Chronic ITP 四、(Operation) Splenectomy
五、BMT(bone marrow transplantation) • SAA • MDS
Laboratory findings in anaemia Drs Shepherd, Dexter, and Rapson Spring 2001
Scanning Electron microscopy: normal red cell