MSc CogNeuro
MSc CogNeuro. Lecture 1-2: Intro + Primary Motor Cortex (MI) www.psychol.ucl.ac.uk/patrick.haggard/MSC/msc_1.ppt. Action. Behaviour Movement Cognition Survival. Brain control to action. Not conscious Computational processes Learning. Computational process. Volition I want to do X

MSc CogNeuro
E N D
Presentation Transcript
MSc CogNeuro Lecture 1-2: Intro + Primary Motor Cortex (MI) www.psychol.ucl.ac.uk/patrick.haggard/MSC/msc_1.ppt
Action • Behaviour • Movement • Cognition • Survival
Brain control to action • Not conscious • Computational processes • Learning
Computational process • Volition I want to do X • Selection How will I do X? • Initiation Start to do X • Execution Movement towards… • Monitoring Have I got there yet… • Stopping Deactivate X • NOTE: Process is serial, hierarchical, and information expansion
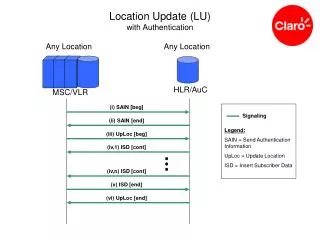
motor command Goal/ Intention Limb Planner (Inverse model) efference copy Forward model sensory feedback Computational model of action control(Blakemore, Wolpert, Frith, Trends in Cognitive Science, 2002)
Provisional Road Map (PH) • A backwards hierarchy • (Muscle) • Primary motor cortex • Premotor cortex (preparation) • Supplementary motor area (physiology, psychology) • Basal Ganglia (physiology, neurology) • Cerebellum (physiology, neurology) • Cortical association circuits (somatosensory, social)
Layered structure of cortex • Descending output from layer 5 • (pronounced in cortex) • Layer 4 absent • Betz/pyramidal cells
Fine-grained local somatotopy in MI is quite fractured/overlapping • Several MI zones produce same movement when stimulated • Perhaps each movement is represented once for each task or synergy? We don’t know…
Rathelot & Strick (2006). Muscle representation in the macaque motor cortex: An anatomical perspective. PNAS, 103, 8257-8263
Rathelot & Strick (2006). Muscle representation in the macaque motor cortex: An anatomical perspective. PNAS, 103, 8257-8263
Lateral corticospinal tract (Pyramidal tract) Fine motor control of contralateral muscles Kuypers (1968) Corticomotoneuronal cell: 1 synapse from muscle - Cell body in MI, leaves via pyramidal tract
Lawrence & Kuypers 1968 • Pyramidal tract lesion • Removes key output from MI direct to muscles • Lasting deficit in fine finger movement
Primary motor cortex code for muscle force. Evarts et al., 1968
Lemon 1988. Spike triggered averaging • 1 MI cell contributes to force in several muscles (one-many mapping) • Task-specificity • 1 MI cell drives a given muscle in task A but not in task B • Looks smarter than a marionette!
Graziano et al (2002) • Micro-stimulate right M1 (and towards PMC) • Long stimulation (behavioural timescale) • Postures independent of start position • Defensive ‘sensory-relevant’ postures
“Somatotopic map” is in fact a functional map of different types of manual behaviour • Pro: sensorimotor transformation, motor equivalence, inverse model • Con: artificial, not physiological, M1 with amputated inputs!
Population coding in MI? • Each neuron broadly tuned for direction • Multiple neurons in population • Population vector predicts movementdirection • (Georgopoulos et al., 1998)
Additional topics • Task specificity of MI neurons • Relation to somatotopy • MI lesions in man • Hemiplegia • Psychological consequences: anosognosia for plegia • Right hemisphere lesions • Probably requires parietal damage also
Anosognosia • RH damage • MI AND Temporoparietal junction