Download
1 / 36
360 likes | 432 Views
Explore the efficiency of capitation vs. fee-for-service for Medicaid patients with severe mental illness. This study compares costs, outcomes, and cost-effectiveness to guide resource allocation effectively.

E N D
Cost-effectiveness analysis of capitation vs. fee-for-service for Medicaid patients with severe mental illnessRichard GrieveVisiting scholar UC BerkeleyLondon School of Hygiene and Tropical Medicine
Joint work-Acknowledgments • Jasjeet Sekhon • Dept Political Science, UC Berkeley • Tei-wei Hu, Joan Bloom • School of Public Health UC Berkeley
Content of talk • Applied study • Context • Methods • Results • Discussion • Key Methodological issue
Context to the study • Worldwide concerns about cost of health care • How best to deploy scare resources to improve population health? • Cost-effectiveness analysis (CEA) technique for guiding resource use towards efficient allocation (Gold et al, 1997) • Some governments routinely use CEA to set priorities (UK, Australia, Canada) • Its use is controversial, and its uptake variable (Sheldon et al 2002)
Context to the study • Lack of explicit use of CEA in US (Neuman et al 2006) • Concerns about rationing of resources (Aaron et al 2005) • Historically concern about methodological standards (Prosser et al 1996, Gold et al 1997) • How to value outcomes (QALYs) • How to represent uncertainty • Published evaluations tend to report costs and outcomes separately, rather than present full CEA
Context: Case study • FFS vs capitation for Medicaid cases with severe mental illness • Studies found capitation associated with lower costs • e.g. Bloom et al 2002; Lurie et al 1992 • Clinical outcomes similar (Cuffel et al 2002) • Studies report costs and outcomes separately • Unclear whether capitation is more cost-effective? • Specific Aim of this study: to demonstrate use of CEA for assessing relative cost-effectiveness • Illustrate by conducting CEA of capitation vs FFS for Medicaid cases with severe mental illness
Methods: case study overviewsee Bloom et al (2002) • Legislation passed in Colorado in 1995 • Medicaid services for patients with mental illness • Counties divided into 3 groups • Group 1:FFS • Group 2: Direct Capitation (DC) • Group 3: Managed care Behavioral Organizations (MBHO) • Observational study focused on severe mental illness • Compared costs and outcomes across 3 groups • Before and after introduction of capitation
Methodsdefinition of ‘interventions’ • FFS: providers reimbursed retrospectively • DC: Community mental health services (CMHC) contract with state to organize/provide services • Not for profit • MBHO • Joint venture between for profit private firm commissioning services • CMHCs provided some services • State regulation/ audit • Contracts every 2 yrs
Methodsselection of groups • In population • CMHCs in each county bid for capitation contract • State selected those bids perceived to be ready • In Evaluation • those counties most comparable • A stratified random sample of cases • Data for analysis for 522 cases across 3 groups
Methodscost and outcome measurement • Costs and outcomes measured over 3 nine month periods • Cost measurement • Medicaid costs claims data, shadow billing • Considered substitution of health services • Outcome measurement • Short form 36 (SF-36); global functioning (GAF) • Outcome valuation • Brazier et al (2002) • QALY calculation: utility score* life years
MethodsAnalytical strategy • Baseline differences in casemix, cost and health status • Used non-parametric method to match cases • Genetic matching algorithm (Diamond and Sekhon 2006, Sekhon 2006, Mebane and Sekhon 1998) • Applied Multivariate matching across 3 groups using • Previous costs; baseline costs, baseline outcomes, casemix
Analytical strategy • Reported incremental QALYs and costs separately • Reported incremental cost-effectiveness • Reported incremental net benefits (INB) • INB (A vs B)=λ(ΔE)-ΔTC • λ-societal willingness to pay health gain • ΔEi and ΔTCi mean difference in effects and costs • if INB>0 then ‘accept’ A in preference to B • Test whether conclusions vary according to λ • Plot cost-effectiveness acceptability curves • Probability ‘intervention’ is cost-effective
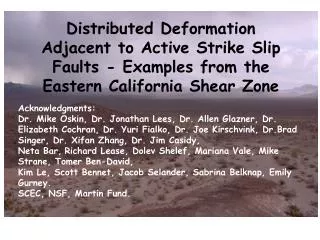
Results: baseline imbalanceMean costs ($) FFS vs MBHO before and after matching (9 month period) For FFS n=151 before and after matching, MBHO=195 before and n=151 after matching KS test: Bootstrap Kolomogorov-Smirnov test
Results: Mean utility and mean QALYs QALYS: FFS vs DC p=0.48; FFS vs MBHO p=0.30
ResultsMean Cost per case ($) over each 9 month period costs: FFS vs DC p=0.06; FFS vs MBHO p=0.32
‘conclusions’ from cost-consequence • DC significant increase in cost vs FFS • MBHO non significant decrease vs FFS • No significant outcomes differences • Can we make use of evidence? • CEA
Cost-effectiveness analysis (over 18 months)means (95% CI)* λ =$50,000 per QALY gained; * bootstrapped bias corrected version
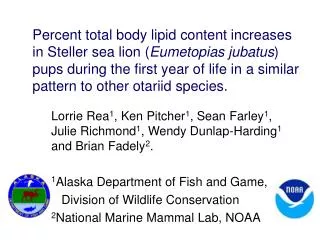
Role of cost-effectiveness analysis DC vs FFS MBHO vs FFS
Preliminary conclusions from CEA • Cost effectiveness analysis useful in extending traditional cost-consequence approach • Allows for potential tradeoffs between costs and outcomes • In this case study/context CEA found that: • MBHO model more cost-effective than FFS • DC model less cost-effective than FFS (or MBHO) • Observational study but results based on appropriate methods adjusting imbalance • Sensitivity analysis applied 2 part model to adjust for any outstanding differences: findings unchanged
Why the difference? • MBHO model- for profit stronger incentive to cost minimise • Interviews (Bloom et al 2000) suggested MBHO emphasised maintaining access but reducing costs per user • DC areas had less targeted utilisation review • Different capitation models targeted different patient groups
Conclusions in context of other findings • Caveats • small nos, Short followup • selection centres • Only sub sample severe mental illness • limited to morbidity costs • Other analyses found capitation associated with cost reductions without selection (Coffman et al 2006, wallace et al 2006) • Addition to literature suggesting form of capitation matters
Methodological extensionsuse of appropriate methods correcting for imbalance • Lack of use of appropriate matching methods in health services research • Deeks et al (2003) highly critical of current methods of bias adjustment in observational studies • Seriously limits their use in policy making • Economic evaluations often dependant on data from observational studies • Rely on ‘traditional’ methods of casemix adjustment • Recent interest in use of propensity score methods in cost-effectiveness analysis (Mitra et al 2005) • More work in other areas e.g. labour economics
Methods to adjust for baseline differences • Genetic matching • Improves on alternative methods such as multiple linear regression and propensity scores • More efficient even when propensity score is known • When propensity score is unknown • Genetic matching minimizes bias even where • distribution of baseline measures are skewed, • covariates have non linear relationship with outcomes
A more general solutionGenetic matching (GM) algorithmDiamond and Sekhon (2006) • Uses search algorithm (Mebane and Sekhon 1998) • On basis of stringent non-parametric tests of balance searches for ‘best’ match between treatment and controls across baseline covariates • Previous work demonstrated that when applied to observational data can replicate the results of RCTs • Software now available- Sekhon 2006
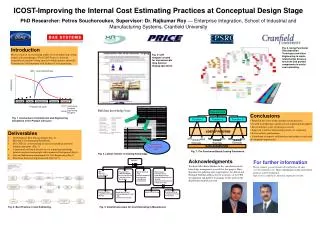
Baseline cost imbalance for FFS vs MBHO comparison:pre and post matching
Comparison of method for adjusting for baseline imbalances • Compare cost-effectiveness estimates • from unmatched data with parametric model adjusts using mean differences (1) • from unmatched data with parametric model adjusts using linear adjustment (2) • From matched data with parametric model adjusts using linear adjustment (3) • Parametric model uses 2 stage and log transform
Preliminary conclusion for methodological section • unbiased estimates of cost-effectiveness important • Choice of method can make a difference • Inappropriate method of adjustment overstated probability intervention was cost-effective • Genetic matching preferable does not rely on assumptions routinely violated • Skewed cost data, non linear relationships • Method works well even for this smallish case study because of baseline data on costs, outcomes and casemix • Further applications are required