Download
1 / 19
190 likes | 359 Views
Musculoskeletal & Biomechanical Adaptations to Training HPER 6310. Dr. Suzan Ayers Western Michigan University. Lecture Overview. Effects of Physical Activity on: bone joints and ROM muscle-tendon units body size, shape & composition Biomechanical Adaptations to Training: muscular

E N D
Musculoskeletal & BiomechanicalAdaptations to Training HPER 6310 Dr. Suzan Ayers Western Michigan University
Lecture Overview Effects of Physical Activity on: • bone • joints and ROM • muscle-tendon units • body size, shape & composition Biomechanical Adaptations to Training: • muscular • neuromuscular Biomechanical Adaptations to Injury
Physical Activity & Bone • Disuse results in osteopenia (bone loss) • Genetically determined baseline mass for normal function (certain level of PA to ↔ bone health) • ↓ PA=bone loss, ↑ PA=bone growth (see below) • Weight-bearing PA= bone growth • Too much intense PA problematic; optimal levels exist for each individual
Physical Activity & Joints/ROM • Short-term effects of cyclical exercise (bike, run) • Articular cartilage thickens (improved force dissipation) • 2-3x ↑ in volume of synovial fluid in a joint (lubricant) • Evidence supports endurance exercise’s benefits over sprint training on ligament strength • Degenerative joint disease (osteoarthritis) • Thinning articular cartilage • Thickening compact bone under articular cartilage • Possible genetic, aging & environmental factors impact DJD dev’t • Regular runners do NOT have > incidence of osteoarthritis HMMMM…
Physical Activity & Muscle-Tendon Units • Flexibility: The ability to move a joint through its complete range of motion (ROM) (ACSM, 2000) • depends on muscle-tendon units crossing joints • is joint-specific • ↑ flexibility related to ↑ extensibility of connective tissue • strength and flexibility training can promote ↑ ROM • Laxity: The degree of abnormal motion of a given joint (Heyward, 2002) • ↑ injury risk • Hypermobility: Excess ROM at a joint (Heyward, 2002)
Active • Self-stretching • Passive • Partner provides force of stretch • Static • Slow, sustained stretch held for 10-30 sec • Preferred in Physical Education settings • PNF (Proprioceptive Neuromuscular Facilitation) • Combo active/passive techniques • NOT for children 6-10 yrs • Ballistic/Dynamic • Quick movements, bouncing, using momentum • Reserve for those 15+ yrs • Helpful to prepare athletes for competition
Static stretches should be held to the point of mild discomfort “No pain, no gain” is INAPPROPRIATE! • Training principles • Frequency: Daily (min 3x/wk) • Intensity: To point of mild discomfort • Time: 10-30 sec • Type: Static, PNF, partner, etc.
Strength changes • Weeks 6-8 primarily neuromuscular • Weeks 9+ gains due to ↑ fiber size/volume • Long-term benefits • Fiber changes resulting in improved fatigue-resistance • ↑ relative amount of connective tissue Tendon Adaptations • Much slower rate of adaptation than muscle • Collagen synthesis ↑ • Fibers align more regularly longitudinally • Muscle strains often occur @ junction of tendon and muscle
Physical Activity’s Effect on Body Size, Shape & Composition Endomorph relaxed, sociable, tolerant, comfort-loving, peaceful, plump, buxom, developed visceral structure Mesomorph active, assertive, vigorous, combative, muscular Ectomorph quiet, fragile, restrained, non-assertive, sensitive, lean, delicate, poor muscles
Dr. William Sheldon’s “somatotypes” Endomorph Mesomorph Ectomorph
Somatotype challenge In the 1940s, Dr. William Sheldon (1898-1977) proposed a theory about how certain body types ("somatotypes") are associated with certain personality characteristics. He claimed that there are three such somatotypes: endomorphy, mesomorphy, and ectomorphy. You can rate yourself on each of these three dimensions using a scale from 1 (low) to 7 (high) with a mean of 4 (average). Therefore, a person who is a pure mesomorph would have a score of 1-7-1. A pure endomorph would be 7-1-1. A pure ectomorph would score a 1-1-7. A mostly average person who has some endomorphic tendencies would have a score of 6-4-4 ... etc. Rate the degree to which you think you possess each of the three body types.
Endomorphic Body Type • soft body • underdeveloped muscles • round shaped • over-developed digestive system Associated personality traits: • love of food • tolerant • evenness of emotions • love of comfort • sociable • good humored • relaxed • need for affection
Mesomorphic Body Type • hard, muscular body • overly mature appearance • rectangular shaped • thick skin • upright posture Associated personality traits: • adventurous • desire for power and dominance • courageous • indifference to what others think or want • assertive, bold • zest for physical activity • competitive • love of risk and chance
Ectomorphic Body Type • thin • flat chest • delicate build • young appearance • tall • lightly muscled • stoop-shouldered • large brain Associated personality traits: • self-conscious • preference for privacy • introverted • inhibited • socially anxious • artistic • mentally intense • emotionally restrained
Lifestyle Factors • ↑ PA while ↓ caloric intake=fat loss • Training can make physiological changes at any age (it’s never too old to teach an old dog new tricks • Height is genetically predetermined • Weight can be altered to a given genetic point • Somatotype can change as strength and endurance requirements change
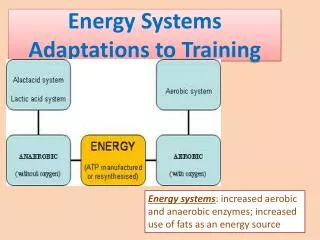
Biomechanical Training Adaptations • Training influences both contractile properties of muscle (strength, speed) and neural control (coord.) • Strength changes due to • ↑ net neural drive to muscle (motor unit recruitment) • ↑ muscle size • both neural and structural changes • Contraction speed changes due to • Δ in shape of muscle’s force-velocity curve • Δ in value of the intrinsic max shortening velocity • both shape and max shortening velocity changes
Muscular Training Adaptations • Max force produced depends on length of muscle during contraction • Initial strength gains (wk 2-8) primarily neural • 10+ wk gains primarily hypertrophic • Isokinetic training can change force-velocity curve • Contraction speed changes also influence force-velocity curve shape, ergo power (strength x speed = power)
Neuromuscular Training Adaptations Incidence of serious knee injury 6x F>M athletes • Intrinsic risk factors for ACL injury • Lower extremity malalignment • ↓ intercondylar notch width at the knee • ↑ knee joint laxity • Hormonal influences (Relaxin) • Extrinsic risk factors for ACL injury • Imbalanced quad/ham strength • Inadequate neuromuscular control GOAL: improve stability (balance, coordination), proprioception, & strength
ACL injury-prevention neuromuscular programs • Knee stability/function improve with ↑ in postural equilibrium, intermuscular control & leg muscle strength • Means of ↑ aforementioned factors: • Stretching • Plyometric exercises (AKA, jump training) • Weight lifting • Evidence supporting neuromuscular training’s role in ↓ incidence of sport-related knee injuries • Ham:Quad strength ratio key to ACL injury prevention • Neuromuscular training can ↑ knee joint stability • ↑ H:Q • Fine-tune neural control over hamstrings