Download

1 / 18
180 likes | 300 Views
The Child Development Program (CDP) outpatient reform project aimed to enhance patient care continuity and reduce waiting times by integrating General Practitioner (GP) services in the referral process. Over two years (2009-2010), the project identified key issues in communication and collaboration between specialists and GPs. With input from UQ, protocols were developed to streamline referrals, gather service utilization data, and establish a GP liaison role. Results included reduced waiting times from over 12 months to 10 weeks and positive feedback from both GPs and specialists.

E N D
Outpatients reform in the Child Development Program 01March 2012
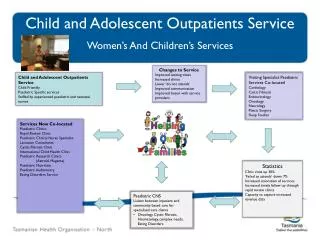
GP – Specialist Outpatient Project • Project Scope • 2 Year Project (2009 -2010) • Evaluation partner – UQ • Services in scope • Royal Brisbane & Women’s Hospital • Urology Outpatients • Ophthalmology Outpatients • Royal Children’s Hospital • Paediatric ENT • Child Development Program
GP – Specialist Outpatient Project • Aim of the project: • To assign GPs to work with outpatient services to: • Understand issues faced by staff and specialists in OPD clinics • Review current referral & discharge processes • Provide a GP perspective on referral and discharge processes • Collaboratively work toward reducing waiting list. • Achieve better continuity of patient care
Child Development Program • GP Advisor - Dr Dana Newcomb • Benchmarking nationally with services in Sydney, Melbourne, Perth, Gold Coast and Brisbane. • Literature review on child development shared care models • Interviews with senior CDP staff (Brisbane, Gold Coast, Sydney • Identification of issues contributing to long waiting lists
Issues Identified • Referral process • Lack of trust/understanding of roles • Internal processes
Referral Process GP Parent CDU Teacher Assessment of Referrals Other GP Referral Required
Lack of Trust & Understanding of Roles • Specialists did not discharge patients • Poor communication between specialists and GPs • Generally poor collaboration between CDP and GPs • Lack of GP knowledge about developmental disorders • Lack of GP awareness of other community resource options • Poor collaboration between Community Child Health Nurses and GPs
Internal Processes • New patients were required to be seen by the specialist prior to receiving any allied health services. • Wait times refer to the time waiting to see the specialist. • Wait times for allied services vary, but generally relatively lengthy.
Development of a GP Liaison Role • GP Liaison Officer - Lesley Martin • Work with the GP Advisor to: • Develop protocols which support Shared Care Model • Define referral guidelines • Maximise use of Information Technology • Identify alternative community resource options • Develop an early identification tool • Collect service utilisation data
Data Collection • Clinical diagnostic data was collected over a three month period to discern the highest primary diagnoses with a view to service planning • Austistic Spectrum Disorder • Pervasive Developmental Disorder as a secondary diagnosis • Intellectual impairment 50% of referrals in that time related to speech and language concerns of 0-2yr olds.
Outputs, Resources & Tools • The Red Flag Early Intervention Guide for children 0 – 5 years. • eReferral template developed • Clear referral guidelines published • Centralized referral assessment process • Feedback to GP process introduced • Dedicated GP phone number • Intake officer – alternate options • GP Liaison – 116 GP visits to 47 practices
Outcomes: Referral Process GP Parent CDU Teacher Assessment Report Assessment of Referrals Other
Outcomes • GP phone line utilised - 41% of phone calls received were from GPs. • 96% of GPs Surveyed were positive about the changes • Waiting times were reduced from over 12 months to 10 weeks
GP Perspective • Positive feedback from GPs • Laminated Red Flag Resource displayed in Practices/Treatment rooms • Practice visits well received • GP referrals more qualitative and inclusive of pre-determining factors • Secure messaging - direct referral link to central Clinical Intake at CDP
Paediatric Specialists’ Perspective • Raised awareness of GP role • Increased confidence to transfer review patients to GP care • Letters to GPs have become more structured • Recognition of enhancements achieved through electronic communication • Paediatric representation on Shared Care Working Party
Patient Perspectives • Improved continuity of care • Clearer referral pathway • More timely response to referral and appointment booking. • Enhanced transition into adulthood for patients with life-long complex developmental difficulties
In Summary • GP input into OPD processes has made a difference to waiting lists • Electronic communication between OPD and GP has streamlined processes • This project has assisted with ongoing service planning
For more details...... • Helen Hoare • Health Service Liaison Manager • Metro North Brisbane Medicare Local • helen.hoare@mnbml.com.au