Push-dose epinephrine
Push-dose epinephrine. EMS Agency training to be reviewed by all accredited paramedics prior to June 1 st , 2019 Thanks to Justin Bramlette for his work on this training. Background. Epinephrine has broad effects on α , β 1 and β 2 receptors, so it is a potent agent to increase:

Push-dose epinephrine
E N D
Presentation Transcript
Push-dose epinephrine EMS Agency training to be reviewed by all accredited paramedics prior to June 1st, 2019 Thanks to Justin Bramlette for his work on this training
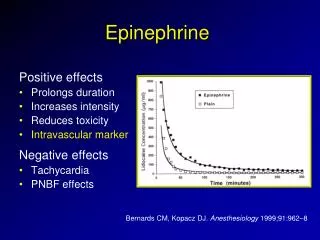
Background • Epinephrine has broad effects onα, β1 and β2 receptors, so it is a potent agent to increase: • Chronotropy (heart rate) and inotropy (myocardium contraction strength) • Vasoconstriction • Bronchodilation • Push-Dose (PD) epinephrine has been used as a quick and easy temporizing vasopressor for years in critical care settings • PD epinephrine is a rapid method to administer a vasopressor • Delivers a dose that is similar to an Epi drip
Warnings! Further literature recommended for general review of push dose pressors: 2018 – The Use of Bolus-Dose Vasopressor in the Emergency Department – Weigand, S, et al 2017 – Bolus Dose of Epinephrine for Refractory Post-arrest Hypotension – Gottlieb, M
When do we use it? Generalized Indications for requesting orders for any vasopressor (dopamine or PD epi): • Hypotension refractory to IV fluids • Most forms of hypotension and shock should have fluids attempted before pressors • Consider requesting orders for pressors prior to completing fluid bolus if • Pulmonary edema is present • Critical hypotension, impending cardiovascular collapse • Consider if Mean Arterial Pressure (MAP) is <45 mmHg • Consider for bradycardia refractory to other causes • Consider reversible causes of bradycardia MAP
When do we use it? • Shock (Medical) (Protocol 619) – Septic Shock, Cardiogenic Shock, Undifferentiated Shock • ROSC with persistent hypotension (Protocol 641) • Bradycardia (Protocol 644) • Neurogenic shock refractory to fluids (Protocol 660) How is it used? • Dosing: • 10mcg/mL (1 mL) IV/IO every 1-3 min • Repeat as needed to maintain SBP >90mmhg • 1 syringe of correctly mixed PD Epi will contain 10 doses! • Base Hospital Order only • If both Dopamine and PD Epi are available make choice between the two in consultation with Base Hospital (until dopamine is phased out)
Protocol #619 - Shock • Hypovolemic Shock - dehydration, GI bleeding, vomiting and diarrhea, etc • Treatment should focus on fluid replacement • Septic Shock - fever, or other symptoms of infection, ALOC, tachypnea • First-line treatment – aggressive fluid replacement (consult base as needed) • Pressors - critical hypotension or shock refractory to fluids • Cardiogenic Shock - cardiac dysfunction, pulmonary edema • Pressors may be considered early • Undifferentiated Shock - uncertain etiology after prehospital assessment • First-line treatment should focus on IV fluids • Pressors - refractory to fluids
Protocol #641Cardiac Arrest (atraumatic) ROSC with Persistent Hypotension • Transient hypotension is common in first minutes after ROSC • Fluid bolus is a reasonable first-line treatment • Consider vasopressors for persistent hypotension • Consider early contact for severe hypotension • Consider early contact if vital signs appear to be deteriorating
Protocol #644Bradycardia • Atropine - First-line treatment for most unstable bradycardias • Pressors – refractory to atropine • Consider early base-contact for orders in unstable high-degree heart blocks • High-degree heart blocks may not respond well to Atropine • 2nd Degree II AVB or Mobitz II • 3rd Degree AVB or Complete Heart Block
Protocol #660Trauma Neurogenic shock • Distributive shock resulting from disruption of the autonomic pathways within the spinal cord • Occurs after damage to the spinal cord or traumatic brain injury • Trauma associated with abnormal motor/sensory exams • Low blood pressure, occasionally with a slowed heart rate • First-line treatment should focus on IV fluids • Pressors - persistent or severe hypotension refractory to fluids MOST hypotension after trauma is caused by hemorrhage which should be treated with permissive hypotension and fluids
Push-Dose Epi Mixing instructions Materials needed Remove vial of Cardiac Epi 1:10,000 (0.1 mg/mL) from box Attach needle to 10mL saline flush
Push-Dose Epi dilution Discharge 1 mL of saline from 10 mL flush giving you 9 mL of saline Draw back 1 mL of air into 10 mL saline flush 1 mL of air 9 mL
Insert needle into vial of Cardiac Epi 1:10,000 (0.1 mg/mL) Inject the 1 mL of air from the saline flush into vial of Cardiac Epi 1:10,000 Draw back 1 mL of Cardiac Epi into the saline flush to get 10 mL of Push-Dose Epi (10 mcg/mL) Push-Dose Epi dilution
Remove needle from PD Epi and mix well. LABEL PD Epi with cloth tape (or other label) marked as Epi 10 mcg/mL. PD Epi 10 mcg/1mL is ready for administration IV or IO, syringe contains 10 doses Push-Dose Epi dilution Epi 10 mcg/mL • Notes Regarding Epi Concentrations: • PD Epi– most dilute, appropriate as vasopressor • 10 mcg/mL = 0.01 mg/mL = 1:100,000 • Cardiac Epi – typically used during cardiac arrest • 1:10,000= 0.1 mg/mL = 100 mcg/mL • IM Epi – NEVER to be used IV/IO in this concentration • 1:1,000 = 1 mg/mL
Push-Dose Epi dilution Alternative mixing instructions • https://www.youtube.com/watch?v=DbHueIqmvnA • Video from Inland Counties EMS Agency • These mixing instructions may be used if equipment is available • Thank you for reviewing these protocols changes • PD Epi protocols may be utilized starting June 1st, 2019 • Dopamine will be phased out of stock on equipment over several months • Updated protocols will be available from link on EMS Agency homepage starting June 1st, 2019 • Sloemsa.org • EMS app update is pending • Contact dbrim@co.slo.ca.us with questions