Download
1 / 63
700 likes | 943 Views
MODERN DIAGNOSIS AND TREATMENT OF LUNG CANCER. Department of Thoracic Surgery, General and Oncology Surgery Medical University in Łódź. Author: M.D. Sławomir Jabłoński. LUNG CANCER EPIDEMIOLOGY. ONE OF THE MOST FREQUENT MALIGNANT NEOPLASMS IN HUMANS FIRST cause of death in males

E N D
MODERN DIAGNOSIS AND TREATMENT OF LUNG CANCER Department of Thoracic Surgery, General and Oncology Surgery Medical University in Łódź Author: M.D. Sławomir Jabłoński
LUNG CANCER EPIDEMIOLOGY ONE OF THE MOST FREQUENT MALIGNANT NEOPLASMS IN HUMANS FIRSTcause of death in males THIRD cause of death in females EUROPE :21% of all cancer cases, 29% of all cancer deaths POLAND NEW CASES 20 000/year DEATHS nearly 20 000/year M:Fratio = 5:1
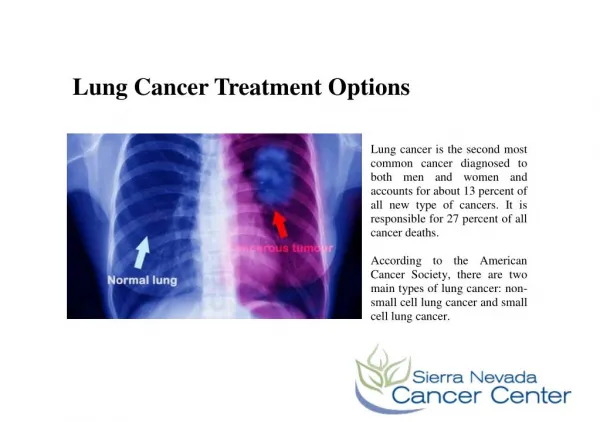
LUNG CANCER -DEFINITION Primary lung cancer is a malignant neoplasm originating from epithelial cells of bronchial tree or other cells of the lung tissue
Lung cancer is divided into two large groups LUNG CANCER NON-SMALL CELL SMALL CELL LUNG CANCER LUNG CANCER 75% 25% PLANOEPITHELIAL CARCINOMA MIXED OAT CELL 50% CARCINOMA ADENOCARCINOMA INTERMEDIATE CELL CARCINOMA 20% LARGE CELL CARCINOMA OAT CELL CARCINOMA 20% MIXED CARCINOMA CARCINOID BRONCHIALVEOLAR CARCINOMA 10%
SMALL CELL LUNG CANCER Definition Small cell lung cancer (SCLC) is a fast-growing type of lung cancer. It tends to spread much more quickly than non-small cell lung cancer. Causes About 15% of all lung cancer cases are small cell lung cancer. Small cell lung cancer is slightly more common in men than women. Smoking almost always causes small cell lung cancer. Small cell is the most aggressive form of lung cancer. It usually starts in the air tubes (bronchi) in the center of the chest. These tumors can rapidly spread to other parts of the body, including the brain, liver, and bone.
SMALL CELL LUNG CANCER - DIFFERNECE Small cell carcinoma is different from the rest of histopathological types of lung cancer because of several biological and clinical features such as: • High speed of proliferation • Short time of duplication of the tumor mass • Early metastases by blood stream • Sensitivity to cytostatic treatment and ionic radiation • Bad outcome of surgical treatment Considering above mentioned features, lung cancer in clinical practise is often simply divided into two groups: • Non-smallcell carcinoma ( NSCC) • Smallcell carcinoma (SCC)
LUNG CANCER – RISK FACTORS CARCINOGENIC FACTORS : SMOKING !!!( 60 times higher risk when smoking > 40cigarettes a day) OCCUPATIONAL RISK FACTORS NICKEL, CHROMIUM, ASBESTOS, ARSENIC HYDROCARBONIC COMPOUNDS RADIOACTIVE METALS ENVIORNMENTAL POLLUTION TUBERCULOSIS AND CICATRICAL CHANGES OF THE LUNG HORMONAL FACTOR ( difference in occurrence in males and females) IMMUNOLOGICAL DEFECTS GENETIC FACTORS ( disorders in chromosome 3, K-ras,HER-2/neu, p53, Rb)
PERIPHERAL CARCINOMA ( often adenoidal carcinoma) CENTRAL CARCINOMA ( growth in large bronchi) LUNG CANCER – CHARACTER OF GROWTH
LUNG CANCER CHARACTER OF GROWTH METASTATIC CARCINOMA ( numerous focal changes in both lungs)
SMALL CELL LUNG CANCER - staging Limited stage Cancer is found only in one lung and in nearby lymph nodes. (Lymph nodes are small, bean-shaped structures that are found throughout the body. They produce and store infection-fighting cells.) Extensive stage Cancer has spread outside of the lung where it began to other tissues in the chest or to other parts of the body. Recurrent stage Recurrent disease means that the cancer has come back (recurred) after it has been treated. It may come back in the lungs or in another part of the body.
NON-SMALL CELL LUNG CANCER TNM STAGING TNM CLASSIFICATION T(tumor feature) TIScarcinoma in situ T1 tumor up to 3cm surrounded by the lung tissue T2 tumor larger than 3 cm, more than 2 cm from tracheal bifurcation. T3 tumor of any size infiltrating the thoracic wall, diaphragm, mediastinal pleura. Tumor less than 2 cm from tracheal bifurcation. T4 tumor of any size infiltrating mediastinum, heart, large vessels, trachea, esophagus, vertebral body, tracheal bifurcation. Presence of neoplastic cells in the pleural liquid.
N1 LYMPHATIC NODES OF HIALUS N2 MEDIASTINAL LYMPHATIC NODES N3 LYMPHATIC NODES OF THE OPPOSITE SIDE AND SUPRACLAVICULAR LUNG CANCER – (N feature positive)
LUNG CANCER – METASTASES (M feature) METASTASES OF THE LUNG CANCER: TOPICAL: ANATOMICAL STRUCTURES OF MEDIASTINUM PLEURA THORACIC WALL REGIONAL LYMPHATIC NODES: LUNG HIALUS - N1 MEDIASTINAL - N2 HIALUS OF THE OPPOSITE LUNG – N3
LUNG CANCER – METASTASES (M feature) • VISCERAL METASTASES : • HEPAR • BRAIN • BONES, BONE MARROW • SUPRARENAL GLANDS • SUBCUTANEOUS TISSUE
T2 tumor larger than 3 cm, more than 2 cm from tracheal bifurcation.
T3 tumor of any size infiltrating the thoracic wall, diaphragm, mediastinal pleura. Tumor less than 2 cm from tracheal bifurcation.
T4 tumor of any size infiltrating mediastinum, heart, large vessels, trachea, esophagus, vertebral body, tracheal bifurcation. Presence of neoplastic cells in the pleural liquid.
CLINICAL ASSESSMENT OF LUNG CANCER PROGRESSION CLINICAL GRADES OF PROGRESSION • Grade 0 Tis N0 M0 GOOD • Grade IA T1 N0 M0 RESULTS • Grade IB T2 N0 M0 OF SURGICAL • Grade IIAT1 N1 M0 TREATMENT • Grade IIBT2 N1 M0, T3 N0 M0 • Grade IIIA T1 N2 M0, T2 N2 M0, T3 N1 M0, T3 N2 M0 • Grade IIIB every T N3 M0, T4 every N M0 • Grade IV every T, every N, M1
LUNG CANCER DIAGNOSTICS SUBJECT EXAMINATION HISTORY: • FAMILY OCCERRENCE OF NEOPLASM • EXPOSITION TO SMOKE FROM CIGARETTES • OCCUPATIONAL EXPOSURE
LUNG CANCER DIAGNOSTICS SUBJECT EXAMINATION SYMPTOMS DEPENDENT ON PRIMARY TUMOR AND TOPICAL EXPANSION OF NEOPLASM • COUGH (CHANGE OF COUGH IN SMOKERS) • HEMOPTYSIS • DYSPNOEA • PAIN IN THE CHEST • RECURRENT OR LONG-LASTING PNEUMONIA • HOARSENESS • DYSPHAGIA • SHOULDER PAIN
LUNG CANCER DIAGNOSTICS SUBJECT EXAMINATION GENERAL SYMPTOMS: • OSTEOARTICULAR PAINS • GENERAL WEAKNESS • LOSS OF BODY MASS • INCREASE IN BODY TEMPERATURE • OTHER SYMPTOMS OF PARANEOPLASTIC SYNDROMES
LUNG CANCER DIAGNOSTICS PHYSICAL EXAMINATION (we can identify) • WORSENING OF BRONCHIAL PATENCY • ENLARGEMENT OF LYMPHATIC NODES • PLEURAL EXUDATE • PERICARDIAL EXUDATE • SUPERIOR CAVAL VEIN SYNDROME • HEPAR ENLARGEMENT • THROMBOPHLEBITIS • PAIN IN THE CHEST ON PRESSURE • PARANEOPLASTIC SYNDROMES • OCCUPATION OF CENTRAL OR PERIPHERAL NERVOUS SYSTEM
LUNG CANCER • CLINICAL SUSPICION OF HIGH PROGRESSION OF LUNG CANCER: • CLINICAL SYMPTOMS: • hoarseness (palsy of recurrent laryngeal nerve, infiltration on aortic arch) • enlargement of supraclavicular lymphatic nodes ( occupation of N3 nodes) • superior caval vein syndrome ( tumor infiltration or pressure of packet of enlarged lymphatic nodes on a superior caval vein) • neurological symptoms ( metastases in brain)
LUNG CANCER • SUSPICION OF HIGH PROGRESSION OF LUNG • CANCER: • EXAMINATION RESULTS: • in X-ray – atelectasis of the whole lung • presence of neoplastic cells in pleural liquid ( T4 feature ) • in bronchoscopy infiltration of tumor < 2 cm from tracheal bifurcation • shoulder pain ( Pancoast tumor – neoplasm originating from lung apex infiltrating ribs, subclavicular vessels, shoulder plexus or spine) • enlargement of the lymphatic nodes of N2 or N3 group in CT
PARANOEPLASTIC SYNDROMES They are a group of clinical symptoms of the neoplasm resulting from secretion of substances of different biological effects by the neoplasms and not connected with direct influence of the tumor or metasteses on the neighboring tissues. Clinical symptoms manifest in about 50% of patients. • Anorexia-cachexia syndrome (the most frequent) • Hypertrophic pulmonary osteoarthropathy (bilateral edema and osteoarticular pains of forearms and shanks) • neuropathies and encephalopathies in patients without metastatic changes in nervous system, Eaton-Lambert pseudomiasthenic syndrome • Skin changes – so called revelators of the neoplastic disease ( dermatomyositis, lupus erythematosus, acanthosis nigricans, sclerodermia) • Hypercoagulability of blood and wandering thrombophlebitis + other hematological disorders (anemia, thrombocytopenia) • Ectopic secretion of ACTH syndrome (up to 20% of patients with Cushing syndrome) • Incorrect secretion of hormones syndromes – antidiuretic hormone (ADH), parathormone (hiperkalcemia), serotonin (carcinoid syndrome) and others
DIAGNOSTICS OF LUNG CANCER EXAMINATIONS USED TO ASSESSMENT OF PROGRESSION OF LUNG CANCER: SUBJECT AND PHYSICAL EXAMINATION CHEST X-RAY CHEST COMPUTER TOMOGRAPHY (CT) ULTRASOUND EXAMINATION OR CT OF ABDOMEN CT OR MR (MAGNETIC RESONANCE) OF BRAIN SCYNTYGRAPHY OF BONES POSITRON EMISSION TOMOGRAPHY (PET)
DIAGNOSTICS OF LUNG CANCER INVASIVE EXAMINATIONS - ASSESSMENT OF PROGRESSION OF LUNG CANCER : • BRONCHOFIBEROSCOPY • TRANSESOPHAGEAL OR TRANSBRONCHIAL ULTRASOUND EXAMINATION • MEDIASTINOSCOPY • MEDIASTINOTOMY • BIOPSY OF SUPRACLAVICULAR LYMPHATIC NODES ( DANIELS BIOPSY) • VIDEOTHORACOSCOPY • DIAGNOSTIC-THERAPEUTIC THORACOTOMY
Mediastinoscopy Mediastinoscopy is a surgical procedure to examine the inside of the upper chest between and in front of the lungs (mediastinum). During a mediastinoscopy, a small incision is made in the neck just above the breastbone or on the left side of the chest next to the breastbone. Then a thin scope (mediastinoscope) is inserted through the opening. A tissue sample biopsy can be collected through the mediastinoscope and then examined under a microscope for lung problems, such as infection, inflammation, or cancer.
CLASSICAL RADIOLOGICAL EXAMINATIONS Changes observed in radiograms: ROUND SHADOW OF THE LUNG CHANGE OF OUTLINE OF HILUS AND/OR MEDIASTINUM LOCAL DISORDERS IN AIRITY OF LUNG TISSUE INFILTRATION CHANGES OF LUNG TISSUE COMPUTER TOMOGRAPHY Possibilities of examination: Assessment of location, size and consistency of the tumor Assessment of the neighboring lung tissue Primary assessment of mediastinal lymphatic nodes Assessment of occupation of neighboring organs ( thoracic wall, large vessels, esophagus, diaphragm, pericardium) DIAGNOSTICS OF LUNG CANCER
DIAGNOSTICS OF LUNG CANCER • PRIMARY TUMOR ASSESSMENT: • ENDOSCOPY OF THE BRONCHIAL TREE (location of tumor, distance from carina, state of lymphatic nodes of bifurcation, possibility of taking biopsy specimens to histopathological examination) • RADIOLOGICAL EXAMINATIONS ( classical X-ray, CT, NMR) • CYTOLOGICAL EXAMINATION OF LIQUID FROM PLEURAL OR PERICARDIAL CAVITY ( positive result treated as T4 feature)
DIAGNOSTICS OF LUNG CANCER • ASSESSMENT OF REGIONAL LYMPHATIC NODES : • ENDOSCOPY OF BRONCHIAL TREE (BAC OF TRACHEAL BIFURCATION LYMPHATIC NODES) • RADIOLOGICAL EXAMINATIONS (CT, spiral CT, NMR) • MEDIASTINOSCOPY (NODES OF GROUP II, IV, VII) • PARASTERNALMEDIASTINOTOMY (NODES OF GROUPV i VI ON THE LEFT) • TRANSESOPHAGEAL OR TRANSBRONCHIALULTRASOUND EXAMINATION • DANIELS BIOPSY of suprasternal lymphatic nodes • VIDEOTHORACOSCOPY
DIAGNOSTICS OF LUNG CANCER • ASSESSMENT OF ORGAN METASTASES : • ULTRASOUND EXAMINATION OR CT OF ABDOMEN • THIN-NEEDLE ASPIRATION BIOPSYof suspicious isolated tumor in suprarenal gland • CT or NMR of brain • PET – positron emission tomography • SCYNTYGRAPHY OF OSSEOUS SYSTEM (routine in microcellular carcinoma in planned combined treatment, in non-microcellular carcinoma in case of suspicion of metastases in bones) • BILATERAL TREPANOBIOPSY OF BONE MARROW FROM ILIAC ALA (in microcellular carcinoma in planned combined treatment) • SURGICAL BIOPSY of changes suspected of metastases to subcutaneous tissue
DIAGNOSTICS OF LUNG CANCER METHODS OF ESTABLISHMENT OF HISTOPATHOLOGICAL TYPE • CYTOLOGICAL EXAMINATION OF SPUTUM • CYTOLOGICAL OR HISTOPATHOLOGICAL EXAMINATION OF MATERIAL COLLECTED IN BRONCHOFIBEROSCOPY • CYTOLOGICAL EXAMINATION OF PLEURAL EXUDATE • THIN-NEEDLE ASPIRATION BIOPSY of peripheral lung tumor ( transthoracal thin-needle aspiration biopsy – puncture through thoracic wall under control of ultrasound or CT) • THIN-NEEDLE ASPIRATION BIOPSY OF PERIPHERAL LYMPHATIC NODES • HISTOPATHOLOGICAL EXAMINATION OF MATERIAL FROM MEDIASTINOSCOPY, MEDIASTINOTOMY OR VIDEOTHORACOSCOPY • DIAGNOSTIC THORACOTOMY
TREATMENT OF SMALL CELL LUNG CANCER The basic therapy of this type of lung cancer is chemotherapy, which expands the lenght of life, alleviates the symptoms and reduces the mass of tumor. Usually due to resistance to medicines remission period after chemotherapy is less than a year. The lack of standardized and commonly accepted scheme of treatment. The most often cisplatin combined with etoposide. LD type(limited to one half of the chest) SIMULTANEOUS RADIO-CHEMOTHERAPY (IF THERE IS NO NEOPLASTIC EXUDATE) X-RAY-therapy: According to Turrisi’s scheme – 2 doses daily 1,5 Gy with 6 h break. Total dose 45 Gy in 3 weeks Chemotherapy – 4 cycles lasting 3 days repeated every 3 weeks According to Arriagda’s scheme – alternating chemo radiotherapy, where radiation is applied between 2/3, 3 /4 and 4/5 cycle of chemotherapy. Total radiation dose 55 Gy, altogether 6 cycles of chemotherapy, 7-day breaks ED type(diffuse – the illness expands on the other side of the thorax, mediastinum and supraclavicular nodes) SYSTEMIC, MULTITHERAPEUTIC CHEMOTHERAPY Sometimes preservative radiation of skull, which delays brain metastases in patients with LD type.
TREATMENT OF NON-MICROCELLULAR LUNG CANCER I GRADE: IA (T1N0M0), IB ( T2N0M0) The treatment of choice is surgical resection. Preferably lobectomy , cancer exceeding main Fissurerequire pneumonectomy. T2 tumors from lobal bronchus or infiltrating main bronchus require sleevelobectomy orpneumonectomy. After resection of tumor T1N0M0 5-year survival is estimated to 65-70%, T2N0M0- 45-55% . Perioperative death rate about 3%-4%. In patients disqualified from surgical treatment – radiotherapy recommended. II GRADE: IIA (T1N1M0), IIB ( T2N1M0, T3N0M0) Indicated surgical treatment even with metastases in N1 nodes. Usually anatomical resection of the lung + resection of infiltration on the thoracic wall + lymphadenectomy. Due to frequent local recurrences and visceral metastases additional treatment is recommended; X-ray therapy decreases the frequency of topical and mediastinal recurrences, chemotherapy reduces systemic recurrences. However, no strategy increases total life length. After resection of tumor T1N1M05-year survival is estimated to 45-55%, in T2N1M0-35%-50%. In T3N0M0 tumors about 30%-35%. This group involves tumors of lung apex ( Pancoasta), in which the prognosis is the worst. Preoperative X-ray therapy reduces the mass of the tumor and increases the ability of resection of Pancoast tumors. Preoperative chemotherapy is examined. Only 20% of patients is in I and II grade of progression at the time of diagnosis.