Hypnotics
Jonathan Emens, M.D. Sleep Medicine Clinic Sleep and Mood Disorders Laboratory Oregon Health & Science University Portland, OR. Hypnotics. OPA March 3, 2007. Disclosure.

Hypnotics
E N D
Presentation Transcript
Jonathan Emens, M.D. Sleep Medicine Clinic Sleep and Mood Disorders Laboratory Oregon Health & Science University Portland, OR Hypnotics OPA March 3, 2007
Disclosure None of my slides, abstracts and/or handouts contain any advertising, trade names or product–group messages. Any treatment recommendations I make will be based on best clinical evidence or guidelines.
Outline • Review of Sleep Physiology • Epidemiology of Insomnia • Morbidity in Insomnia • Diagnoses in Insomnia • Hypnotics
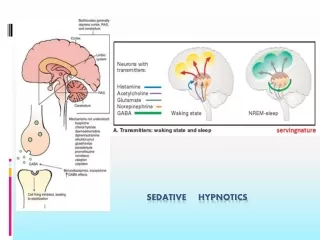
Brief review of Sleep • Reversible, unresponsive state
Brief review of Sleep • Reversible, unresponsive state • Divided into two states: NREM and REM
Brief review of Sleep • Reversible, unresponsive state • Divided into two states: NREM and REM • NREM: Divided into 4 stages based on EEG patterns
EEG in NREM Sleep From: Kryger, Roth, Dement, eds., Principles and Practice of Sleep Medicine, 2005
EEG in NREM Sleep From: Kryger, Roth, Dement, eds., Principles and Practice of Sleep Medicine, 2000
EEG in NREM Sleep From: Kryger, Roth, Dement, eds., Principles and Practice of Sleep Medicine, 2005
EEG in NREM Sleep From: Kryger, Roth, Dement, eds., Principles and Practice of Sleep Medicine, 2005
Brief review of Sleep • Reversible, unresponsive state • Divided into two states: NREM and REM • NREM: Divided into 4 stages based on EEG patterns • REM: distinct EEG, muscle atonia, rapid eye movements, dreams, PGO waves (measured in animals)
Sleep Staging • Stage 1: 2-5% From: Kryger, Roth, Dement, eds., Principles and Practice of Sleep Medicine, 2000
Sleep Staging • Stage 1: 2-5% • Stage 2: 45-55% From: Kryger, Roth, Dement, eds., Principles and Practice of Sleep Medicine, 2000
Sleep Staging • Stage 1: 2-5% • Stage 2: 45-55% • Stage 3: 3-8% From: Kryger, Roth, Dement, eds., Principles and Practice of Sleep Medicine, 2000
Sleep Staging • Stage 1: 2-5% • Stage 2: 45-55% • Stage 3: 3-8% • Stage 4: 10-15% From: Kryger, Roth, Dement, eds., Principles and Practice of Sleep Medicine, 2000
Sleep Staging • Stage 1: 2-5% • Stage 2: 45-55% • Stage 3: 3-8% • Stage 4: 10-15% • REM: 20-25% From: Kryger, Roth, Dement, eds., Principles and Practice of Sleep Medicine, 2000
REM and NREM patterns • First third of the night mostly NREM, especially stage 3 and 4 (slow wave) sleep
REM and NREM patterns • First third of the night mostly NREM, especially stage 3 and 4 (slow wave sleep) • Last third of the night mostly REM sleep
REM and NREM patterns • First third of the night mostly NREM, especially stage 3 and 4 (slow wave sleep • Last third of the night mostly REM sleep • Cycles of NREM and REM sleep occur every 90-110 minutes
REM and NREM patterns • First third of the night mostly NREM, especially stage 3 and 4 (slow wave sleep) • Last third of the night mostly REM sleep • Cycles of NREM and REM sleep occur every 90-110 minutes • Amount of slow wave sleep (SWS) decreases with age (greater decreases in men)
Changes in Sleep with Age Ohayon M, et al. Sleep. 2004;27:1255-1273.
Memory impairment surrounding sleep onset From: Kryger, Roth, Dement, eds., Principles and Practice of Sleep Medicine, 2000
Insomnia Definitions • “difficulty in initiating and/or maintaining sleep.” – International Classification of Sleep Disorders (ICSD) • Difficulty Falling Asleep • Difficulty maintaining sleep • Early morning awakening • Daytime fatigue, poor concentration, and irritability
Epidemiology of Insomnia • Depends on Definition: 4.4-48% prevalence in general population Ohayon M, Sleep Med Rev. 2002;6: 97-111.
Epidemiology of Insomnia • Depends on Definition: 4.4-48% prevalence in general population • Insomnia Symptoms: 30-48% Ohayon M, Sleep Med Rev. 2002;6: 97-111.
Epidemiology of Insomnia • Depends on Definition: 4.4-48% prevalence in general population • Insomnia Symptoms: 30-48% • Insomnia Symptoms > 3 times/week or “often” or “always”: 16-21% Ohayon M, Sleep Med Rev. 2002;6: 97-111.
Epidemiology of Insomnia • Depends on Definition: 4.4-48% prevalence in general population • Insomnia Symptoms: 30-48% • Insomnia Symptoms > 3 times/week or “often” or “always”: 16-21% • Insomnia Symptoms that are “moderate” or “severe”: 10-28% Ohayon M, Sleep Med Rev. 2002;6: 97-111.
Epidemiology of Insomnia • Depends on Definition: 4.4-48% prevalence in general population • Insomnia Symptoms: 30-48% • Insomnia Symptoms > 3 times/week or “often” or “always”: 16-21% • Insomnia Symptoms that are “moderate” or “severe”: 10-28% • Insomnia Symptoms with Daytime sequelae: 9-15% Ohayon M, Sleep Med Rev. 2002;6: 97-111.
Epidemiology of Insomnia • Depends on Definition: 4.4-48% prevalence in general population • Insomnia Symptoms: 30-48% • Insomnia Symptoms > 3 times/week or “often” or “always”: 16-21% • Insomnia Symptoms that are “moderate” or “severe”: 10-28% • Insomnia Symptoms with Daytime sequelae: 9-15% • Dissatisfaction with amount or quality of sleep: 8-18% Ohayon M, Sleep Med Rev. 2002;6: 97-111.
Epidemiology of Insomnia • Depends on Definition: 4.4- 48% prevalence in general population • Insomnia Symptoms: 30-48% • Insomnia Symptoms > 3 times/week or “often” or “always”: 16-21% • Insomnia Symptoms that are “moderate” or “severe”: 10-28% • Insomnia Symptoms with Daytime sequelae: 9-15% • Dissatisfaction with amount or quality of sleep: 8-18% • Insomnia Diagnosis (DSM-IV): 4.4-11.7% (many with symptoms don’t meet DSM criteria) Ohayon M, Sleep Med Rev. 2002;6: 97-111.
Epidemiology of Insomnia • 5,622 subjects Ohayon M, J Psychiatr Res. 1997;31:333-346.
Epidemiology of Insomnia • 5,622 subjects • 18.7% had complaints of difficulty initiating or maintaining sleep or of non-restorative sleep Ohayon M, J Psychiatr Res. 1997;31:333-346.
Epidemiology of Insomnia • 5,622 subjects • 18.7% had complaints of difficulty initiating or maintaining sleep or of non-restorative sleep • 12.7% had sleep complaints for > 1 month that caused “clinically significant distress or impairment” Ohayon M, J Psychiatr Res. 1997;31:333-346.
Epidemiology of Insomnia • 5,622 subjects • 18.7% had complaints of difficulty initiating or maintaining sleep or of non-restorative sleep • 12.7% had sleep complaints for > 1 month that caused “clinically significant distress or impairment” • 10.3% with Axis I or II disorder Ohayon M, J Psychiatr Res. 1997;31:333-346.
Epidemiology of Insomnia • 5,622 subjects • 18.7% had complaints of difficulty initiating or maintaining sleep or of non-restorative sleep • 12.7% had sleep complaints for > 1 month that caused “clinically significant distress or impairment” • 10.3% with Axis I or II disorder • 1.3% primary insomnia Ohayon M, J Psychiatr Res. 1997;31:333-346.
Epidemiology of Insomnia • 5,622 subjects • 18.7% had complaints of difficulty initiating or maintaining sleep or of non-restorative sleep • 12.7% had sleep complaints for > 1 month that caused “clinically significant distress or impairment” • 10.3% with Axis I or II disorder • 1.3% primary insomnia • 0.5% general medical condition Ohayon M, J Psychiatr Res. 1997;31:333-346.
Epidemiology of Insomnia • 5,622 subjects • 18.7% had complaints of difficulty initiating or maintaining sleep or of non-restorative sleep • 12.7% had sleep complaints for > 1 month that caused “clinically significant distress or impairment” • 10.3% with Axis I or II disorder • 1.3% primary insomnia • 0.5% general medical condition • 0.3% circadian disorder Ohayon M, J Psychiatr Res. 1997;31:333-346.
Morbidity/Co-Morbidity • Objective cognitive/performance deficits? Ford DE and Kamerow DB, JAMA. 1989;262:1479-1484. Mellinger GD et al., Arch Gen Psych. 1985;42:225-232. Kryger, Roth, Dement, eds., Principles and Practice of Sleep Medicine, 2005
Morbidity/Co-Morbidity • Objective cognitive/performance deficits? • Quality of life: subjective deficits in memory, concentration, & work performance Ford DE and Kamerow DB, JAMA. 1989;262:1479-1484. Mellinger GD et al., Arch Gen Psych. 1985;42:225-232. Kryger, Roth, Dement, eds., Principles and Practice of Sleep Medicine, 2005
Morbidity/Co-Morbidity • Objective cognitive/performance deficits? • Quality of life: subjective deficits in memory, concentration, & work performance • Psychiatric: prevalence of any psychiatric disorder is 2-3x greater in insomniacs, depression prevalence is 4x greater Ford DE and Kamerow DB, JAMA. 1989;262:1479-1484. Mellinger GD et al., Arch Gen Psych. 1985;42:225-232. Kryger, Roth, Dement, eds., Principles and Practice of Sleep Medicine, 2005
Morbidity/Co-Morbidity • Objective cognitive/performance deficits? • Quality of life: subjective deficits in memory, concentration, & work performance • Psychiatric: prevalence of any psychiatric disorder is 2-3x greater in insomniacs, depression prevalence is 4x greater • Medical: insomnia associated with multiple medical conditions; increased HD risk & impaired immune function? Increased mortality rates? –confounding factors. Ford DE and Kamerow DB, JAMA. 1989;262:1479-1484. Mellinger GD et al., Arch Gen Psych. 1985;42:225-232. Kryger, Roth, Dement, eds., Principles and Practice of Sleep Medicine, 2005
Morbidity/Co-Morbidity Chang PP, Am J Epidemiol. 1997;146:105-114.
Morbidity/Co-Morbidity Weissman MM, Gen Hosp Psych. 1997;19:245-250.
Differential Diagnosis • Psychiatric • Medical • Neurological • Environmental • Circadian Rhythm Disorder • Primary Sleep Disorder: sleep apnea, PLMs & restless legs syndrome, & parasomnias • “Behavioral”: inadequate sleep hygiene • Stress related transient Insomnia • “Primary Insomnias”: psychophysiological insomnia, sleep state misperception, & idiopathic insomnia (no primary insomnia in ICSD vs. DSM) From: Kryger, Roth, Dement, eds., Principles and Practice of Sleep Medicine, 2000
Treatment • Treat underlying Medical Condition • Treat underlying Psychiatric Condition • Improve sleep Hygiene • Change environment • CBT: “primary insomnias”, transient insomnia • Pharmacological • Light, melatonin, or “chronotherapy” for Circadian disorders
Treatment • Treat underlying Medical Condition • Treat underlying Psychiatric Condition • Improve sleep Hygiene • Change environment • CBT: “primary insomnias”, transient insomnia • Pharmacological • Light, melatonin, or “chronotherapy” for Circadian disorders
“Hypnotics” • Benzodiazepine Receptor Agonists (BzRAs) • Benzodiazepines • Non-Benzodiazepines GABAA agonists • Sedating Antidepressants • Sedating Antipsychotics • Antihistamines • Gamma-Hydroxybutyrate (GHB) • Melatonin and Melatonin agonists, Gabapentin, Valerian
BzRAs • Benzodiazepines, zaleplon, zolpidem, zopiclone, & eszopiclone • All act on gamma-aminobutyric acidA (GABAA) benzodiazepine receptor complex • Preoptic area of anterior hypothalamus?
GABAA benzodiazepine receptor complex • 5 glycoprotein subunits • Each subunit may have multiple forms • Benzodiazepine binding is inhibitory by increasing frequency of Cl- channel opening From: Kryger, Roth, Dement, eds., Principles and Practice of Sleep Medicine, 2005