Download
1 / 65
800 likes | 2.53k Views
Delayed Puberty – A Disorder in Timing????. Kristy Parker PGY-2 Pediatrics December 4 th , 2009. CanMEDS Objectives. Medical Expert 1. Outline the normal physiology, progression, and timing of pubertal development. 2. Delineate causes of delayed puberty in both the male and female.

E N D
Delayed Puberty – A Disorder in Timing???? Kristy Parker PGY-2 Pediatrics December 4th, 2009
CanMEDS Objectives Medical Expert • 1. Outline the normal physiology, progression, and timing of pubertal development. • 2. Delineate causes of delayed puberty in both the male and female. • 3. Explain how to differentiate between constitutional delay and other causes of delayed puberty. Manager • 1. Outline appropriate investigations for male and female patients with delayed puberty.
Assessment of Puberty History • Parents • Important to ask about onset of puberty in parents • Menarche (more reliable in mothers as they remember onset) • Male growth spurt (as most fathers recall their pubertal progression more vaguely) • Age of first shaving regularly • Parental heights (identify midparental height) • “late bloomer” vs. “early bloomer” • Body changes? (important to ask about EACH) • Thelarche (galactorrhea) • Adrenarche/pubarche (body odor, axillary & pubic hair, acne) • Menarche • Gonadarche
History cont’d… • Important to include: • Past medical history (history of brain tumor, radiation, chemotherapy, known genetic disorder, chronic disease affecting growth) • Eating habits • Any evidence of disordered eating • Activity level • Is exercise excessive or is this an athlete with a high level of training • Growth history • Previous growth chart can be extremely helpful
History • Review of Systems • CNS: visual changes/visual field abnormalities, headaches, anosmia • Cardiac: congenital anomaly • Respiratory: asthma • Renal: • GI: diarrhea, blood in stools
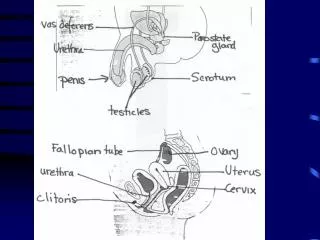
Physical Examination • Examination of Growth • Height • Weight • Head circumference • Upper to lower segment ratios • Pubertal Assessment (Tanner staging) • Axillary hair • Pubic hair & staging • Breast development & staging • Genital development & staging • Neurological assessment CPS position statement on growth measurment
Tanner Staging of Puberty in Males • Tanner I • prepubertal (testicular volume less than 3.5 ml; small penis of 3 cm or less) [typically age 9 and younger] • Tanner II • testicular volume between 1.6 and 6 ml; skin on scrotum thins, reddens and enlarges; penis length unchanged [9-11] • Tanner III • testicular volume between 6 and 12 ml; scrotum enlarges further; penis begins to lengthen to about 6 cm [11-12.5] • Tanner IV • testicular volume between 12 and 20 ml; scrotum enlarges further and darkens; penis increases in length to 10 cm and circumference [12.5-14] • Tanner V • testicular volume greater than 20 ml; adult scrotum and penis of 15 cm in length [14+]
Tanner Pubic Staging Pubic hair (both male and female) • Tanner I • no pubic hair at all (prepubertal Dominic state) [typically age 10 and younger] • Tanner II • small amount of long, downy hair with slight pigmentation at the base of the penis and scrotum (males) or on the labia majora (females) [10–11.5] • Tanner III • hair becomes more coarse and curly, and begins to extend laterally [11.5–13] • Tanner IV • adult-like hair quality, extending across pubis but sparing medial thighs [13–15] • Tanner V • hair extends to medial surface of the thighs [15+]
Tanner Breast Development Breasts (female) • Tanner I • no glandular tissue; areola follows the skin contours of the chest (prepubertal) [typically age 10 and younger] • Tanner II • breast bud forms, with small area of surrounding glandular tissue; areola begins to widen [10-11.5] • Tanner III • breast begins to become more elevated, and extends beyond the borders of the areola, which continues to widen but remains in contour with surrounding breast [11.5-13] • Tanner IV • increased breast size and elevation; areola and papilla form a secondary mound projecting from the contour of the surrounding breast [13-15] • Tanner V • breast reaches final adult size; areola returns to contour of the surrounding breast, with a projecting central papilla. [15+]
Normal Pubertal Physiology • HPG axis (hypothalamic-pituitary-gonadal) is essential in turning on puberty at appropriate times • Pulsatile secretion of GnRH is essential • GnRH is produced in hypothalamus (in arcuate nucleus) • GnRH travels to the anterior pituitary to stimulate the production of LH & FSH
Normal Pubertal Physiology • HPG axis is active in the first few weeks of life • LH & FSH rise as hCG from placenta is gone • This results because the fetoplacental unit acts to produce negative feedback on the HPG axis during late gestation • HPG axis usually quiescent during childhood • Result of negative feedback on the hypothalamus • Axis re-stimulated during adolesence • Stimulation results in a positive feedback loop (estrogen from maturing follicle stimulates LH surge for ovulation) • Pulsatile release of hormone increases overnight first. This eventually progresses to secretion during day and night. LH can be detected in pulsatile forms. FSH has longer half-life, so pulses not as evident • Menarche does not signal full maturation of HPG axis (may simply be withdrawl bleeding from progesterone -> cycle takes longer to become ovulatory
Role of Gonadotropins • FSH • Stimulates androstenedione by the ovary • Involved in spermatogenesis in the testes • Induces receptors for LH • LH • Uses androstenedione for substrate to produce estradiol in theca cells • Stimulates testosterone synthesis by Leydig cells • FSH is usually higher than LH in prepubertal stages, and this reverses in pubertal stages
Age of Pubertal Progression • Females • Thelarche • Generally considered the onset of puberty • Occurs in most girls at 9.5-10.4 • Menarche • Mean age of onset = 12 yrs • Adrenarche • Usual onset at approx age 9.4-10.6 yrs • Linear Growth • Generally occurs before Tanner Stage 2 breast development • Generally adds 20-25cm of height in females • GH increases during puberty as well (provides 50% of growth spurt) (NHANES III dates)
Are females entering puberty earlier? • Onset of puberty earlier, but completion has not changed • Differences between ethnic groups • ? Related to environmental factors or food additives • ? Related to better nutritional status, increased body mass/adiposity
Pubertal Progression • Males • Gonadarche • Testicular enlargement generally heralds the onset of puberty (testes > 4ml). This usually starts around 10.8-11.1 yrs. • Initial increases in testicular size are due to increase in Sertoli (supporting cells) • Average time to complete genital development = 3yrs • Thelarche • 2/3 of males will have gynecomastia develop during puberty (midpubertal) • Gynecomastia results from direct testicular secretion of estrogen as well as peripheral conversion of prohormones to estrogen • Pubarche • Linear growth • Peak growth generally occurs after Tanner Stage 5 • Generally adds 25-30cm in height for males
http://psycnet.apa.org/journals/bul/110/1/images/bul_110_1_47_fig2a.gifhttp://psycnet.apa.org/journals/bul/110/1/images/bul_110_1_47_fig2a.gif
Role of Bone Age • Comparing radiographs of hand & wrist to reference standards • Female skeletal maturity is generally 2 yrs advanced as compared to males • Pubertal events more correlated with bone age than chronological age
Psychological Effects • Puberty occurs during adolescence during time of identity formation • Period of increased physical changes • When teens are behind their peers in terms of development, can lead to substantial teasing/bullying & self-esteem issues
Jameson, J.L. Rites of passage through puberty: A complex genetic ensemble. PNAS. October 30, 2007. Vol 104, No. 44.
NR0B1 gene is involved in development & function of the adrenal gland & HPG axis for gonadotropin secretion • GPR54 gene mutations affect GnRH release (these patients do respond to exogenous GnRH) • PROP1 mutations lead to problems in differentiation of gonadotropicc, somatotropic, lactotropic & thyrotropic cells.
Pubertal Delay • Based on statistical norms (>2 SD from the population mean) • Pubertal delay is most often seen in males • Present far more often than females as delay causes more significant psychosocial implications • Most commonly no pathology present
Timing of Puberty • Consider pubertal delay if: • No breast development by age 13 in a female • No menses by age 15 in a female • Testicular size < 2.5cm or 4mL or pubic hair is not present by age 14 in a male • Consider precocious puberty if: • Breast development before age 8 or menarche before age 10 in females • Testes volume > 3ml before 9 years. • Pubic hair development before 8 years in females, and 9 years in males
Pubertal Delay Pubertal Delay Hypogonadotropic Hypogonadism Hypergonadotropic Hypogonadism Eugonadotropic Hypogonadism Low FSH, LH Low sex steroids High FSH, LH Low sex steroids Normal FSH, LH
Pubertal Delay • Sedlmeyer et al. identified in their study that delayed puberty in men could be classified as • Constitutional delay of growth & puberty in 63% • Delay associated with underlying medical condition 20% • Hypogonadotropic hypogonadism 9% • Hypergonadotropic hypogonadism 7%
Hypogonadotropic Hypogonadism • Constitutional Delay of Puberty • Malnutrition • Excessive Exercise • Growth Hormone Deficiency • Isolated Gonadotropin Deficiency • Endocrine Causes • Miscellaneous syndrome complexes • Brain tumors • Craniopharyngioma, astrocytomas, gliomas, histiocytosis X, germinomas, prolactinomas • Iron overload (pituitary damage) • GnRH receptor abnormalities
Constitutional Delay of Puberty • Most common cause of pubertal delay • Delayed puberty often found in siblings or parents • Diagnosis of exclusion • Bone age is delayed & consistent with degree of pubertal maturation (usually delayed by 2yrs or more • Often associated with constitutional short stature
Constitutional Delay of Puberty cont’d… • Progressive height gain, but along lower limits of normal (contrast to isolated gonadotropin deficiency which has normal growth, but no pubertal growth spurt) • Early morning testosterone levels > 0.7nmol/L predict puberty within 15 months (Wu et al)
Constitutional Delay of Puberty cont’d… • Differentiated by pathological gonadotropin deficiency by observation over time (no definitive test available) • GnRH stimulation test occasionally used, but not conclusive • HPG axis responds to GnRH more strongly if it has already been exposed to this (reflects previous stimulation) • hCG stimulation test can also be undertaken (Degros et al) • Stimulated testosterone < 3 nmol/L suggestive of hypogonadotropic hypogonadism • Stimulated testosterone >9 nmol/L suggestive of CDGP
Kallman Syndrome • A syndrome of isolated gonadotropin deficiency • 1/10,000 males, 1/50,000 females • Present with ANOSMIA or HYPOSMIA • Can be difficult to differentiate from constitutional delay • KAL-1 gene encodes protein (anosmin) required for GnRH neurons to migrate from olfactory placode to cribiform plate • Can also be associated with harelip, cleft palate, and congenital deafness
Idiopathic Hypogonadotropic hypogonadism • Males often have eunochoid body proportions (upper-to-lower segment ratio of < 1) • Can be sporadic or familial • Can be related to problems in the receptor for GnRH • Can present as infant with micropenis & cryptorchidism. These infants will not show normal gonadotropin increase in the first few weeks of life
Excessive exercise • Questions as to whether lack of puberty related to low body weight or more as a direct effect of exercise • Interruption of training in ballet dancers, runners
Syndromes Associated with Pubertal Delay • Prader-Willi syndrome • Laurence Moon syndrome • Septo-optic dysplasia • Bardet-Biedl syndrome
Panhypopituitarism • Pubertal delay is usually not presentation (present with short stature earlier)
What controls the timing of puberty? An update on progress from genetic investigations? Current Opinion in Endocrinology. 2009
Hypergonadotropic hypogonadism • Gonadal damage secondary to chemotherapy/radiation • Enzyme defects in the gonads • Androgen insensitivity • Ovarian/testicular dysgenesis (causes of gonadal failure)
Gonadal Failure (bilateral) • In these cases, circulating levels of LH & FSH are high (hypergonadotropic hypogonadism) • Congenital • Turner Syndrome • Klinefelter’s Syndrome • Complete androgen insensitivity • Acquired • Chemotherapy/Radiation/Surgery • Postinfectious (ie. mumps orchitis, coxsackievirus infection, dengue, shigella, malaria, varicella) • Testicular torsion • Autoimmune/metabolic (autoimmune polyglandular syndromes) • “Vanishing Testes syndrome” • “Resistant Ovaries syndomre” (gonadatropin receptor problems)
Klinefelter’s Syndrome • 45 XXY most common (2/3), remainder are mosaic or variant • Many affected boys will not be identified until adolescence when puberty is delayed • Some pubertal development, but testes eventually become fibrotic • Timing relates to degree of mosaicism in the patient • Small testicles & gynecomastia • Also often small phallus size • 90-100% are infertile • More female type fat distribution • Tall in childhood, with euchanoid body habitus • Have fathered children (particularly those with mosaicism)
Turner Syndrome • 45 XO genotype most common • Associated with short stature, variable degrees of puberty, primary amenorrhea & multiple congenital anomalies • Often presenting complaint is short stature, but in others, may present with delayed puberty • Most have primary ovarian failure • 50% of patients have some breast develpoment, some axillary/pubic hair is typical for most patients • Associated with SHOX mutations which cause the short stature
Turner syndrome cont’d… • Residual ovarian function can cause breast development in 15-25%, menarche in 5-10% & pregnancy in 1-3%
Receptor Defects • LH gene defects and FSH gene defects can result in high levels of FSH & LH with low sex steroids • Secondary sex characteristics are driven by LH effects, can have FSH receptor defect & normal secondary sex characteristics
Eugonadotropic pubertal delay • Congenital Anatomic Anomalies • Imperforate hymen • Vaginal atresia • Vaginal aplasia • PCOS • Hyperprolactinemia