
Understanding Acute Cholangitis: Symptoms, Diagnosis, and Treatment
E N D
Presentation Transcript
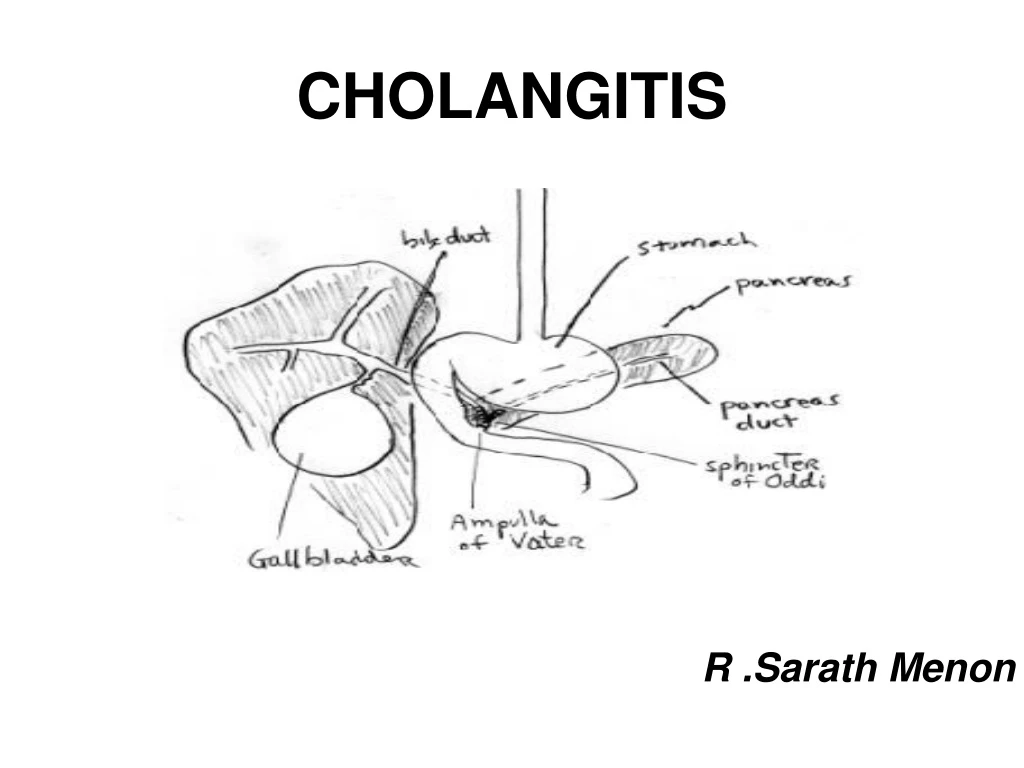
CHOLANGITIS R .Sarath Menon
ACUTE ( Bacterial) Suppurative Non Suppurative • Sclerosing Cholangitis
Definition • Inflammation of the bile ducts • Bacterial infection
History • By Jean-Martin Charcot in 1877 • Charcot triad • Reynolds & Dargan – Reynolds pentad
Pathophysiology • Biliary tract obstruction • Elevated intraluminal pressure • Infection of bile
Etiology • Choledocholithiasis • Malignant Strictures • Benign Strictures • Indwelling Tubes or Stents • Cholangiography • Parasitic • Ischaemia • Chemicals
Bacteriology Gram Negative Pathogen • E-coli (25-50%) • Klebsiellae Pneumonia (15-20%) • Enterobacter Species (5-10%) Gram Positive Pathogen • Enterococcus (10-20%)
Bacteriology • Bacteria are present on bile culture in approximately 75% patients with acute stage • Patients with common duct stones have a higher probability of positive bile culture than those with gallstones in the gallbladder or cystic duct
Bacteriology Some features of bacteria that may enhance pathogenicity in this setting include: • External pili in Gram negative Enterobacteria, which facilitate attachment to foreign surfaces such as a stone or stent. • A glycocalyx matrix composed of exopolysaccharides produced by bacteria which protect the organisms from host defense mechanisms and may hinder penetration of antibiotics.
Symptoms • Biliary colic pain: episodic RUQ or epigastric abdominal pain that begins abruptly, is continuous, resolves slowly and lasts for 30 minutes to 3 hrs • Jaundice • Spiking fever with chills • Nausea and vomiting may precipitate by fatty food
Symptoms • Charcot’s triad: • Biliary colic pain • Jaundice • Spiking fever with chills • Reynold's pentad • Charcot’s triad + mental confusion + hypotension:often suggested severe septicemia (only present in about 50% cases)
Differential Diagnosis • Cholecystitis and Biliary Colic • Diverticular Disease • Hepatitis • Mesenteric Ischemia • Pancreatitis • Shock, Septic
Laboratory Data • WBC elevated with neutrophil predominance • A cholestatic pattern of liver function test • Abnormalities with elevations in the serum Alk-P gammaglutamyl transpeptidase (GGT), and bilirubin (predominantly conjugated) concentration. • Serum amylase can be increased to three to four times normal, suggesting an associated pancreatitis.
Laboratory Data • Pattern of acute hepatocyte necrosis can be seen in which the aminotransferases may be as high as 1000 IU/L. This pattern reflects microabscess formation in the liver. • Blood cultures should be performed in all patients in whom cholangitis is suspected. • Cultures should also be obtained from bile or stones
Investigations 1. Hepatobiliary Ultrasound • initial screen for investgating the possible biliary tract obstruction
Indicated for evaluation of hepatic or pancreatic masses 2. Abdominal CT
Magnetic resonance cholangiopancreatography Contraindication: Claustrophobia and certain metals (iron) • Excellent sensitivity for biliary duct dilatation, biliary stricture, and intraductal abnormality • Identify pancreatic duct dilatation or stricture, pancreatic duct stenosis
V: gall bladder G: Common bile duct P: Pancreatic duct M: stomach D: duodenum
Endoscopic retrograde cholangiopancreatogram (ERCP) • Contraindication: Pregnancy, Acute pancreatitis, severe cardiopulmonary disease • Indicated : ---when absence of dilated ducts (Ex; PSC) ---suspected pancreatic, ampullary or gastroduodenal disease ---prior biliary surgery ---For Endoscopic sphincterotomy
Endoscopic retrograde cholangiopancreatogram (ERCP) Best visualization of distal biliary tract • Bile or pancreatic cytology • Endoscopic sphincterotomy and stone removal • Biliary manometry
Endoscopic retrograde cholangiopancreatogram (ERCP) • Complication of ERCP: • Pancreatitis • Cholangitis, sepsis • Infected pancreatic pseudocyst • Perforation • Hypoxemia, aspiration
Percutaneoustranshepatic cholangiogram ( PTCD) Contraindication: Pregnancy, Uncorrectable coagulopathy, massive ascites • Indication: when ERCP is contraindicated or failed ---best visualization of proximal biliary tract --- to get bile cytology, culture and for drainage
Treatment • Antibiotic treatment :for nonsuppurative cholangitis • Ampicillin + Gentamicin • Meropenem • Quinolones (Levofloxacin)
Treatment • Toxic cholangitis • ICU • Vasopressors • IV Fluids • Antibiotics
Treatment • Emergency biliary decompression • Endoscopically • Percutaneous transhepatic
Treatment • Proximal Perihilar ObstructionorBiliary – Enteric anastomotic stricture • Percutaneous drainage • Endoscopic • Sphincterotomy • Stone Extraction • Stent
Surgical Care • CBD Exploration • T-tube drainage
Pyogenic liver abscess Acute renal failure Complications
Prognosis • Old age • Female • Acute renal failure • Preexisting cirrhosis • Malignant biliary obstruction
Primary Sclerosing Cholangitis • Primary sclerosing cholangitis is a chronic cholestatic disorder characterized by inflammation, fibrosis, and stricturing of medium and large ducts in the intrahepatic and extrahepatic biliary tree • 50-70% of affected individuals are men with mean age of 40 at diagnosis
Pathophysiology • Genetic predisposition : B8 or DR3 • Immunulogic causes • Bacterial toxic damage • Viral infection • Smoking behavior • Biliary arteriolar injury
Clinical Manifestations • Also, can have fever, chills, nights sweats, RUQ pain • Fatigue and pruritis common presenting symptoms • Most patients asymptomatic at time of diagnosis
Laboratory tests • Usually liver tests reveal a cholestatic pattern • Serum Alk phos and BR may fluctuate because of stricture • Serum aminotransferases usually < 300
Imaging most important step ERCP and percutaneous transhepatic cholangiography are gold standard MRCP quite reliabe Early in the disease stage, might only see fine or deep ulceration fo the common bile duct Diagnosis
Disease related complications • Fatigue and pruritis • Metabolic bone disease • Peristomal Variceal Bleeding • Symptomatic choledocholithiasis • Dominant stricture • Cholangiocarcinoma • Colonic dysplasia and carcinoma
TREATMENT • Prednisolone-jaundice • Sx- preop.cholangiography • Stenotic segment exicision & biopsy • Anastomosis • Stents • Liver Transplantation – Only Curative